
Foreword
Ten years ago, A glass half-full was published by the Local Government Association (LGA). Authored by Jane Foot and Trevor Hopkins it quickly became one of the most requested and downloaded reports ever produced by the LGA. It is still being read ten years later.
So why was it so successful? Partly it was timing. In 2010 a possible move of public health back into local government was already being discussed. Since the move in 2013, local authorities and their public health teams have been on a journey together to understand how they can use councils’ traditional functions in conjunction with their newly acquired public health expertise to maximise the contribution to closing the unjust health inequalities gap.
In the foreword to the original report the then Chairman of the LGA Wellbeing Board, Councillor David Rogers stated, ‘The health and wellbeing of our communities falls far beyond the scope of the NHS. Local government has risen to the challenge of working with its communities to improve health and play a leading role in partnership working’. This is more the case now than it has ever been.
An asset-based approach was not new, councillors and community activists, almost instinctively, had been using the principles of asset-based working with their communities for years. However, their methodical use to challenge health inequalities was, and still is, a relatively recent development in the UK. Most councils are embracing community-centred ways of working, but the challenge that many are now seeking to achieve is the scaling-up of a whole-system community-led and asset-based approach.
In his first speech as Prime Minister, Boris Johnson spoke of “levelling up” society. This will require a renewed focus on tackling the health inequalities that exist between and within local authority areas. It’s a stark statistic that almost 20 extra years of healthy life are enjoyed by those in the most prosperous areas of the country, compared with those in the most deprived.
Most importantly it was the values and principles of asset-based working that struck a chord, both in local government and for the individuals, families and communities it serves. The asset-based approach sees citizens and communities as co-producers of health and wellbeing; promotes community networks, relationships and friendships as a way of providing mutual help and support; and, most importantly, empowers communities to control their futures and create tangible resources for themselves. So, what has happened in the ten years since ‘A glass half-full’ was published? What has gone well, and not so well? Are there still challenges to be overcome? What might the future developments and scenarios for adopting this approach be? Most importantly, are the values, principles and themes of asset approaches still relevant in today’s complex and challenging environment?
Fifteen international, national and local practitioners, activists and academics, and both authors of the original report, all experts in asset-based and community-led approaches, have contributed their answers to these questions. These are both stimulating and challenging, even if you do not agree with some of their conclusions or find their analysis accurate or helpful.
As it states in the foreword to ‘A glass half-full’, a healthy debate on these ideas, thoughts and approaches must continue if we are to deal with the health and wellbeing challenges facing us all in the 21st century.

Councillor Ian Hudspeth
Chairman, LGA Community Wellbeing Board
Key messages
Asset-based working needs to be considered at all levels of the system and in a multidisciplinary way to be successful.
Asset-based approaches seek to enhance people’s ability to identify and use their own health resources. This has implications for how professionals and organisations help and support them to do this.
Asset-based working should not be seen as competition to a deficit approach. A focus on deficits like disease should not be abandoned. A focus on assets like resilience is needed to complement the deficit model in order to shift the emphasis to building health rather than just preventing or curing disease.
Language should not get in the way of our need to understand the values and principles on which asset-based models are based.
Learning from practice and sharing experience of what facilitates and hinders success is critical to our ability advance both the conceptual understanding and practical know-how of the asset-approach.
Policy makers need ensure the necessary supportive environments are in place to ensure success. Emphasising the resources, skills and passions of local people can only be realised if communities have a strong economic foundation which supports their ability to engage with programmes that are supposed to help them.
Questioning and challenging power dynamics remains crucial. Those adopting asset-based approaches need to be continually reflective and recognise the challenges inherent in remaining true to the values of community control.
Politicians and senior management should use opportunities, such as financial challenges and devolution, to fundamentally re-think how they could create a new relationship with residents and communities to bring about sustainable public service reform.
Introduction by Antony Morgan, Professor in Public Health, Glasgow Caledonian University
The original paper Revitalising the evidence base for public health: An asset model by myself and Erio Ziglio was published in 2007 in response to the sustained global challenges to reducing health inequalities.
The ‘Asset Model’ was proposed to stimulate discussions within public health about how we could get policy makers, researchers and practitioners to think and act differently in their approach to improving health and wellbeing.
The premise at the time, was that contemporary policy and practice disproportionately emphasised approaches that set out to fix problems (pathogenic or deficit approaches) rather than focusing on what could be gained by working with individuals and communities to make the most of their talents and strengths (salutogenic or asset-based approaches).
However, one paper published in an international journal is not going to change the world. The publication of A glass half-full in 2010 was therefore timely, increasing awareness and deepening debates about how asset-based approaches could be most successfully applied in the UK.
The chapters in this ten-year anniversary publication collectively provide invaluable policy and practice insights from what we have learned since that time; what challenges remain; and what are the current opportunities to be taken to ensure the potential of asset-based approaches is sustained?
The chapters are organised into four themes: policy and structural issues; implementation and organisational change; challenges and critiques; and leadership. Together they reflect the notion that asset-based working needs to be considered at all levels of the system and in a multi-disciplinary way to be successful.
Chapter one draws on the work of internationally renowned experts who introduce some of the key concepts most closely associated with asset-based working.
Firstly, Bengt Lindstrom, introduces the concept of salutogenesis which is often quoted as the overarching idea that underpins asset models. He discusses the concept, initially developed by Israeli American sociologist Aaron Antonovsky, as a means or tool, to enhance people’s ability to identify and use their own health resources. Obviously this has implications for how professionals and organisations help them to do this.
Secondly Erio Ziglio, introduces the concept of resilience and states it as an example of an asset ‘that helps individuals and communities to prepare and anticipate potential future threats or seize opportunities to protect and promote their health and wellbeing’. Ziglio explores the varied aspects of resilience and argues it ‘deserves to be prioritised in programmes and policies that are required to tackle health inequities, promote social justice and human rights’.
Both Lindstrom and Ziglio emphasise that asset-based working should not be seen as competition to a deficit approach. A focus on deficits like disease should not be abandoned, but rather that a focus on assets like resilience is needed to complement the deficit model in order to shift the focus to building health rather than just preventing or curing disease.
In addition to this conceptual evidence base for an asset-approach, chapter one also includes a contribution from Jane South and Jude Stansfield who describe their work to produce the Public Health England (PHE) and NHS England document ‘A guide to community-centred approaches for health and wellbeing’.
Their contribution reinforces the message that by nature ‘community centred approaches are intrinsically asset-based as they seek to build on the range of informal and formal assets within communities and strengthen the factors that create health’. The inference from this, is that language should not get in the way of our need to understand the basic principles on which asset-based models are based. The contribution by South and Stansfield also provides an example of the importance of translating concepts from research into a strategy for taking action.
Chapter two includes a number of contributions that focus on how the asset-based approach has been implemented, both at the level of commissioning and local practice. Janet Harris reflects on what has happened across the commissioning landscape since the publication of ‘A glass half-full’ including a summary of common barriers to asset-based commissioning, as well as offering ‘five steps commissioners can take to be more asset-based’.
Asset-based commissioning sets the framework for asset-based approaches being adopted in practice. South and Stansfield argue that we now have a multitude of practical examples that demonstrate the enthusiasm and commitment to the approach. Importantly these examples collectively offer key insights into the factors that can secure the success of initiatives which utilise the principles of asset-based working. This chapter includes notable examples from Scotland, Leeds and Oldham. Learning from practice by sharing experience of what facilitates and hinders success is critical to our ability to advance both our conceptual understanding and practical know-how of the approach.
Chapter three aims to offer a sense check on the utility and expectations of the asset approach. Shelina Visram, Stephen Crossley and Jennie Popay provide critiques which help to summarise the challenges faced by those trying to put asset-based approaches into practice. One of the key criticisms of the asset-based approach is that it fails to address issues of power and that, particularly in a time of austerity, it could exacerbate growing economic and social inequalities.
Popay argues, that at their worst strength based approaches could help to create a new world of ‘DIY welfare’ at the community level where provision of publicly funded and provided health, social and welfare services recede into the background. The counter argument to this of course, is that one of the key principles of the approach is that all parts of the system need be involved in the process of identifying and utilising assets.
Therefore, by their very nature, policy makers need to ensure the necessary supportive environments are in place to ensure success. Visram and Crossley extend the debates around power, emphasising that the strengths of local people can only be realised if local communities have a strong economic foundation which facilitates their ability to engage with the programmes that are supposed to help them.
The practical examples included in chapter three and throughout the publication provide further examples of current challenges. In sum these contributions reflect the need to continue to take a critical perspective on asset-based approaches and to recognise their limitations.
Asset-based approaches can undoubtedly be used as a cover for handing responsibility for addressing health and social inequities to disadvantaged communities, whilst cutting back on the infrastructure and economic factors that are the root causes of inequities. Questioning and challenging power dynamics remains crucial. Those adopting an asset-based approach need to be continually reflective and recognise the challenges inherent in remaining true to the central value of community control.
Chapter four focuses on the need for culture change, leadership and political commitment as a prerequisite to successful asset-based working. The issues associated with these attributes are illustrated by drawing on the contribution by Councillor Keith Cunliffe and Kate Ardern drawing on their experiences in Wigan.
They describe how the council moved following devolution to a systemwide approach to addressing the challenges the borough faces where community assets are at its heart and how the financial challenges they faced, and the opportunity devolution presented to do things differently in Wigan led to ‘politicians and senior management fundamentally re-thinking how they could create a new relationship with residents and communities’.
They present the principles associated with the ‘Wigan Deal’, an initiative aiming to bring about public service reform. They also present a ‘theory of change’ framework which could help those leading asset-based approaches to understand the process involved in achieving short-, medium- and long-term goals.
Together, the contributions included in this publication demonstrate that a wealth of experience has been gained through the practice of asset-based working over the last ten years. The chapters and case studies also offer ‘a glass half-full’ approach to the challenges by illustrating ways in which policy and practice needs to be shaped to secure a sustained and impactful future for asset-based working.
Background
In early 2019, discussions started with the Local Government Association (LGA) about re-visiting ‘A glass half-full: How an asset approach can improve community health and wellbeing’ published in March 2010. Authored by Jane Foot and Trevor Hopkins it quickly became one of the most requested and downloaded reports ever produced by the LGA. It is still being read and referenced in studies, reports and papers ten years later.
The original report included 10 key messages and it was agreed to ask a number of international, national and local practitioners, activists and academics to review these in the light of developments in health and social care over the last decade. Their contributions are linked to this report and also available as downloads from the LGA website.
These key messages are listed below along with the authors who contributed their analysis and thoughts on these.
The asset approach values the capacities, skills, knowledge, connections and potential in a community. In an asset approach the glass is half-full, rather than half empty."
Erio Ziglio – visiting Professor in Public Health, Glasgow Caledonian University, London
Professor Bengt Lindstrom – Professor of Salutogenesis and Health Promotion, Nordic School of Public Health, Gothenberg
Jane South – Professor of Healthy Communities, Volunteering, Active Citizenship and Community Health, Leeds Beckett University
Jude Stansfield – National Adviser: Public Mental Health, Health Equity and Mental Health
Fundamentally, the shift from using a deficit-based approach to an asset-based one requires a change in attitudes and values."
Mick Ward – Chief Officer, Transformation and Innovation, Adults and Health, Leeds City Council
Lisa Keenan – Commissioning Officer, Adults and Health, Leeds City Council
Professional staff and councillors have to be willing to share power; instead of doing things for people, they have to help a community to do things for itself.’ ‘The values and principles of asset working are clearly replicable. Leadership and knowledge transfer are key to embedding these ideas in the mainstream of public services."
Councillor Keith Cunliffe – Deputy Leader and Cabinet Member for Adult Social Care, Wigan Council
Kate Ardern – Director of Public Health, Wigan Council
Working in this way is community-led, long-term and open- ended. A mobilised and empowered community will not necessarily choose to act on the same issues that health services or councils see as the priorities."
Jennifer McLean – Public Health Programme Manager, The Glasgow Centre for Population Health
Place-based partnership working takes on added importance with the asset approach. Silos and agency boundaries get in the way of people-centred outcomes."
Viola Cassetti – Anthropologist and Development Worker, School of Health and Related Research, The University of Sheffield
The asset approach does not replace investment in improving services or tackling the structural causes of health inequality. The aim is to achieve a better balance between service delivery and community building."
Jennie Popay – Professor of Sociology and Public Health, Lancaster University
Shelina Visram – Institute of Health & Society, Newcastle University
Stephen Crossley – Department of Social Work, Education and Community Wellbeing Northumbria University
One of the key challenges for places and organisations that are using an asset approach is to develop a basis for commissioning that supports community development and community building – not just how activities are commissioned but what activities are commissioned."
Janet Harris – Reader in Knowledge Mobilisation, School of Health and Related Research, The University of Sheffield
Specific local solutions that come out of this approach may not be transferable without change. They rely on community knowledge, engagement and commitment which are rooted in very specific local circumstances."
Carolyn Wilkins – Chief Executive, Oldham Council
A conversation with Jane Foot and Trevor Hopkins
The asset approach values the capacity, skills, knowledge, connections and potentials in a community. In an asset approach, the glass is half-full rather than half empty.”
Our early thinking about developing ‘A glass half-full’ came through a conversation with Antony Morgan who, along with Erio Ziglio, had recently published a very interesting paper setting out a case for action to strengthen health assets in order to improve health, wellbeing and to address inequalities of health.
This paper and our subsequent conversations with Antony and others connected to asset-based approaches led us to think about how we might develop a wider dialogue with local authorities and public health partners that responded to the current state of public health and promoted ideas on community engagement and activism at a local neighbourhood level and the benefits for health and wellbeing.
The message that we have assets, resources, and community networks and a sense of belonging and empowerment… and all those kind of things… we aren’t just deficits, we’re more than that.”
The development of ‘A glass half-full’ came at a time when the public sector was in a cycle of significant change largely shaped by the onset of austerity measures and by structural changes to local government and health – for example the relocation of public health into local government.
There was also an increasing focus on the wider social determinants of health (Fair Society, Healthy Lives: The Marmot Review; Closing the Gap in a Generation Health equity through action on the social determinants of health, WHO Global Commission on Social Determinants) which was shaping not only the discourse but starting to influence policy and practice. Public health practice was stuck in a very individualised and deficit-based way of thinking. There was a new conversation about not just ill-health, but about wellbeing and resilience.
We saw clearly that asset-based approaches and a focus on health assets offered a number of opportunities for local people and public sector agencies. In particular that asset-based approaches are fundamentally ‘place based’ with a focus on generating community energy and action.
This allows people to take control of things that effect their health and build community resources that impact on wellbeing. Councils are responsible for many of the broader determinants of health, for instance housing, schools, the built environment and green spaces, community facilities as well as care services for a range of people.
The asset-based approach provided an opportunity to build on the Marmot Review 2010 and look afresh at what was causing inequalities and how to address the wider determinants of health.
We were setting out a case for the redesign of key services; how the workforce in the public sector could re-orientate to an assets paradigm; and how communities and neighbourhoods could be supported to take action on health and wellbeing through community-led action.
The idea that we can do without public services… that communities, families, neighbours will step in is not one we advocate. We didn’t imagine that when the report was published the social infrastructure that supports people’s lives… community life… the libraries… access to the park and public space… the leisure centre, would be so reduced…"
We were very clear in ‘A glass half-full’, as we are today, that our main aim is not about asset-based approaches as a DIY alternative to properly funded services in communities and neighbourhoods. This is about redirecting services, realigning professional understanding and interventions that recognise what makes people healthy – what creates health.
The report had a strong focus on changing the mind-set of professionals so they would start to recognise that communities have deep reservoirs of knowledge and experience and this could be deployed in re-designing services and informing how resources could be utilised in communities. We believed, and still do, that most people are and have assets as well as deficits; they have something positive to say and contribute. We are starting to see a wealth of asset-based achievements in many places across England and other parts of the UK.
The sense that if you are poor you are helpless and without power; we wanted to recognise that reality but at the same time acknowledge and support action that enabled the voice of people in communities to come to the fore… taking control of their lives to create opportunities to build resilience and strengthen social networks…"
At the time of publishing ‘A glass half-full’ it was helpful to have strong advocates for this approach to challenging health inequalities. Shifting to a new way of doing things alongside people and communities and working to strengthen their networks and knowledge. As the decade has progressed the discourse, the system reform and the evidence base for asset-based approaches has gathered at a pace. We hope that this publication shows the benefits of this approach and why we must continue to invest in it.
We began this journey over a decade ago and we are still convinced that there are many opportunities to shift further towards this approach. Action to tackle the social determinants of health remains essential, but empowering individuals and communities, strengthening civic engagement and promoting participation has a wellbeing dividend for all people in every community.
COVID-19 postscript
The publication of this report was overtaken by COVID-19 which has dominated all our lives for most of 2020 and put public health in the national spotlight. In response we invited our contributors to write a postscript reflecting on how the pandemic has impacted on their conclusions.
The postscripts received can be found added to their full articles on the website. This piece is a summary of the main themes, drawing in addition on further contributions by Jane Foot and Simon Rippon (also on the website).
The over-arching, common theme of the postscripts is that the pandemic has exposed and exacerbated fundamental structural weaknesses in society, while demonstrating how strong individual and community solidarity can be. Another common theme is that the nature of the political and public health response confirms, and makes even more urgent, the need for a shift towards an asset-based, community centred approach.
As Cassetti writes:
“The pandemic has made visible the widening health inequalities between and within countries, as people in more vulnerable situations or living in less advantaged neighbourhoods have been among those worst hit by COVID-19.”
Foot quotes Marmot who points to the “social gradient in mortality rates from COVID-19 – the more deprived the area, the higher the number of deaths. This social gradient is almost exactly paralleled by the social gradient for all causes of death.”
As well as “exposing and exacerbating inequalities” (South and Stansfield), the pandemic has in the UK, as Foot and others argue, exposed the “weaknesses in our public services and our care system.” Ziglio argues that “many lessons on how to increase resilience at system level (which includes 'capacity to transform dysfunctional and obsolete practices’) are sadly learnt from the catastrophic impact of COVID-19.”
But the pandemic has also demonstrated the many assets people and communities have and the strength of community solidarity in extraordinary times. As McLean comments, “the role and significance of community-focused activity and asset-based approaches has never been more important or relevant.” Foot agrees, “strong community networks, neighbourliness and friendship; the benefits of working together and a belief in our own resources have led to and sustained the explosion of mutual aid groups during lockdown.”
Sadly, the upsurge in community responses to the human needs exposed by the virus has been in stark contrast to the UK government's handling of the pandemic. This has been centralised and top down- the total opposite of the 'community-centred public health’ advocated by South and Stansfield.
As Cassetti comments, “previous pandemics have shown, combining evidence-based recommendations with local expertise, can support people in understanding risks and taking up preventive behaviours.” Instead the government has emphasised individual behaviour change with little or no attempt to relate this to local communities.
This happened in part because, up and until the pandemic worsened, the government bypassed public health teams and local authorities, ignoring their local knowledge and expertise and opted instead for a centralised approach. This includes a system of track and trace outsourced at great expense to the private sector.
As Harris states, “national contact tracing was commissioned without any consideration of the international evidence, which shows that using local people, the 'shoe leather' approach, has traditionally been very effective. (There has been) no acknowledgement of what's been done internationally in public health, where other countries use participatory epidemiology, participatory disease surveillance, to involve citizens and mobilise communities.”
As Harris describes, “it is community organisations that have filled the gap, finding volunteers for transport, organising shopping and food deliveries, they have explained what contact tracing is and why we need it. In Sheffield and in other areas the voluntary sector has been instrumental in promoting trust around the process of reporting contacts, staying in contact to help people who test positive and supporting them to shield. They are effective because what they are doing is helping people who may not believe COVID-19 is real, to understand the risks and the reasons for safe behaviour.”
Partnership working has become more critical than ever, Wilkins commenting that in her district of Oldham “never have organisational barriers been so unimportant.”
Yet this together with the rise in community solidarity can be seen as rare positives in the COVID crisis, we should not lose sight, as Popay reminds us, of the fact that, “communities and local groups are filling gaps that would not be there if public services had not been decimated by years of austerity; that the needs communities are trying to meet, including chronic poverty and inadequate housing pre-date the pandemic; and that volunteers are propping up a health and social care system that has long been underfunded and increasingly fragmented.”
In addition, as Rippon points out “health inequalities could increase further if community-based responses are weakest in the most disadvantaged areas and there is no support from other parts of the system.”
As McLean argues, “the role and significance of community-focused activity and asset-based approaches has never been more important or relevant, especially as we start to move into the recovery phase and try to ‘build back better". Contributors suggest the following need to happen:
- Make use of “opportunities for rethinking and developing the relationship between communities and local systems” (Rippon) ensuring “effective community engagement and strong local partnerships with community-based organisations and volunteers” (South and Stansfield).
- “Adequately fund the community and voluntary sector to enable this.” (Harris).
- “Place based commissioning is essential.” (Foot) together with commissioning that is “holistic and responsive” and aligned “to an even greater degree with the support networks that communities have now developed.” (Harris)
As Popay states, “our society after COVID-19 will be even more unequal; the poorest communities will be even poorer, their social and economic assets depleted even further.” As South and Stansfield argue, our response “should not be about piecemeal action, but taking a systematic and scaled approach. It will involve effective co-production with communities at a ‘hyper-local’ or neighbourhood level linked to action on the wider determinants of health, such as housing and poverty, in order to reduce inequalities.
Above all, using a health asset lens in the pandemic and in recovery is about building on what’s there, building up where there are gaps or vulnerabilities and ensuring that the experiences and insights of communities drive public health planning and action.”
It is clear that, “centralised and stand-alone solutions have not worked, cut off as they are from the skills and knowledge held locally” (Foot). The reorientation of the public health system to become community-centred, that South and Stansfield advocate, is needed now more than ever.
Holding up the Mirror - Reflections on community resilience/opportunities for action (Simon Rippon)
The landscape for promoting the wider adoption of asset and community-led approaches that support communities and neighbourhoods in ‘building back better’ health and wellbeing is now well defined. After a decade of austerity measures that had marked impact on a range of inequalities, people and communities are now living with the consequences of the social restrictions implemented as a result of COVID-19. These will be far reaching both in terms of timescale, health status, wellbeing and inequalities in many communities.
There is a growing narrative on how communities of place have responded during the social and economic restrictions in 2020. We read of hyper-local support networks being developed in neighbourhoods to provide social and domestic support to residents.
These ‘mutual aid’ networks have flourished outside the formal structures of public sector organisations such as Local Government and the NHS and to an extent the Voluntary Community Sector infrastructure. I argue that such examples of community organising are to be expected at a time of crisis and are a good example of ‘adaptive resilience’.
We know that Community organising occurs outside of crisis and is something that community members do for a variety of reasons and motivations. During the lockdown period and the restrictions of 2020 I witnessed first-hand how, through my local Council, measures were taken to support and work with mutual aid groups and other place-based groups to galvanise a coordinated response to support people living with vulnerabilities be that in terms of health status, wellbeing or poverty.
For me this all points to a discussion that we need to have locally on how we understand and build community and place-based resilience that has both a health and wellbeing dividend and contributes to tackling inequalities.
This discussion must lead to a range of developmental stages that seek to orientate the system toward a greater emphasis on strengthening health assets, prioritising investment in activities and action that fosters community development and neighbourhood resources that are health promoting. This development needs to be ‘transformative’ enabling people to take greater control and to participate in social action that brings change on inequality, promotes wellbeing and fosters social capital through participating in community life.
In a recent article on resilience with colleagues at Leeds Beckett University we restated the opportunities for developing community resilience through the lens of WHO (Europe) and its place as a key pillar in building health beyond 2020. This four-stage model provides local system leaders, those in communities and organisational sectors, with a clear framework for understanding, articulating and acting on the key stages for building and strengthening resilience, and resilience needs to operate on three levels – with the individual, with the community and across the system.
We need to seek out collaborative opportunities as local system leaders, taking steps to bring together key actors, such as those tasked with public and population health promotion; community building and wider health development – to reflect on the adaptive responses of resilience that were instigated at the time of the ‘lockdown’ phase.
From this there is rich learning that can inform the future anticipatory phase of resilience in communities; engaging a wide range of members from neighbourhoods and communities in this dialogue is critical and underscores a clear asset-based approach.
Such a review should also shape wider systemic transformative action that builds deeper the foundations and architecture with resilient communities, it is also a platform from which to leave behind ‘obsolete practices’ that are not focused on developing resilient community capacity and capability nor congruent to achieving inroads into inequalities that hamper resilience.
In taking steps toward transformative action for resilience the three core steps set out in the Leeds Beckett paper offers an early frame for thinking on action. These are:
- New levels of learning and practice will need to address the interrelationship between different causes of disadvantage within systems if a marked shift is to be made towards resilience and new social infrastructures;
- A health assets approach may provide a useful lens to address inequalities and wider determinants of health such as poor housing, transport and educational attainment.
- Creating opportunities that enable local people and communities to co-design structural change and resources that build a sense of agency and control.
Further steps can include:
- Reorienting key organisational practices to enable community led resources and infrastructure to flourish.
- Design and delivery of local democracy that holds a focus on tackling health and related inequalities (learn from examples of Poverty Commissions)
1. Policy and structural issues
The asset-based approach is built on a sound foundation of concepts and evidence developed from research and from practice. In this chapter we explore some of these concepts before going on to set out a strategic approach developed by Public Health England (PHE) drawing on the key texts written by Bengt Lindstrom, Erio Ziglio, and Jane South and Jude Stansfield.
Underpinning the asset-based model is the concept of salutogenesis, initially developed by Israeli American sociologist Aaron Antonovsky who undertook studies of women who had survived the holocaust and sought to explain how some of them were able to maintain their health and flourish despite their history and experiences.
Lindstrom developed Antonovsky’s ideas further in his paper introducing salutogenesis. He says of the women that Antonovsky studied that they seemed ‘able to use their internal and external resources in a health promoting way. They were able to reflect and draw conclusions based on their earlier life experiences in a new situation and in a flexible way re-orientate their life in a constructive and meaningful direction conducive to overall health’.
Antonovsky called ‘the ability to identify and use one’s health resources’ as having a ‘Sense of Coherence (SOC)’ and Lindstrom argues that it is a ‘key capacity for people´s ability to gain health and have a healthy orientation in life’.
This way of looking at health was new – previously the focus had been on studying what made people ill. It was an important shift from a focus on deficits to a focus on assets; from seeing the glass as half-empty to seeing it as half-full. But as Lindstrom says in his contribution, it is important to emphasise that there remains ‘just as much a need to understand pathology, cure and prevention in combination with salutogenesis as a complement’.
Research into salutogenesis is on-going, wide-ranging and international and there are many related concepts which sit under what Lindstrom calls the ‘salutogenic umbrella’.
{kind=link}
One of these concepts is that of ‘resilience’ which has been developed by Erio Ziglio and others. He describes resilience as ‘a combination of assets, capabilities and positive adaptation that enables people and communities to cope with adversity.
Resilience is an asset that helps individuals and communities to prepare and anticipate potential future threats or seize opportunities to protect and promote their health and wellbeing. As such, strengthening resilience deserves to be prioritised in programmes and policies that are required to tackle health inequities, promote social justice and human rights’.
He concludes that ‘there is now ample evidence that resilience is a key element within what are nowadays commonly referred to as ‘health assets’ and that they operate at the level of community and whole system as well as the individual. Ziglio explores the varied aspects of resilience and emphasises that it helps produce, as well as flourishes in, supportive environments.
Along with Lindstrom he is not saying that a focus on deficits like disease should be abandoned, but rather that a focus on assets like resilience is needed to complement the deficit model and to shift the focus to building health rather than just preventing or curing disease.
But the asset-based approach is about more than the capacity, resilience and skills of people and communities – as it says in ‘A glass half-full’, ‘a health asset is any factor or resource which enhances the ability of individuals, communities and populations to maintain and sustain health and wellbeing’.
This could be the practical skills of community members, their knowledge and connections, the presence of effective community associations, the physical and economic resources of a place, and the resources of community and voluntary sector and statutory organisations available to support a community. An asset-based approach seeks to identify and build on all these assets.
In public health, approaches that aim to build social connections, empower communities and promote greater equity are not new – all build on health promotion knowledge and practice that has been built up in the UK and internationally. The best definition of positive health and wellbeing is derived from the 1986 World Health Organisation (WHO) (Ottowa Charter for Health Promotion.
’Health promotion is the process of enabling people to increase control over, and to improve their health. To reach a state of complete physical, mental and social wellbeing, an individual or group must be able to identify, and realise aspirations, to satisfy needs, and to change or cope with the environment.
Health, is therefore, seen as a resource for everyday life, not the objective of living. Health is a positive concept emphasising social and personal resources as well as physical capacities.' (Ottowa Charter for Health Promotion)
The more recent 2012 WHO report on social determinants of health and the health divide across Europe, Charting the Way to Wellbeing, emphasises the importance of resources and assets to good health. ‘The resilience, capacities and strengths of individuals and communities need to be built on, and the hazards and risks to which they are subjected need to be addressed.’
In their contribution, South and Stansfield describe their work for PHE focused on getting evidence into action to support the uptake of community-centred approaches as part of a strategic approach to improve health and reduce inequalities. The rest of this chapter is taken directly from their contribution.
In addition to the conceptual evidence base for an asset-approach described above South and Stansfield argue that ‘reviews, such as Marmot and Due North - Report of the Inquiry on Health Equity for the North, have provided strong justifications for greater community involvement in decision making, building community capacity and addressing exclusionary processes as part of a social determinants approach to reducing health inequalities.
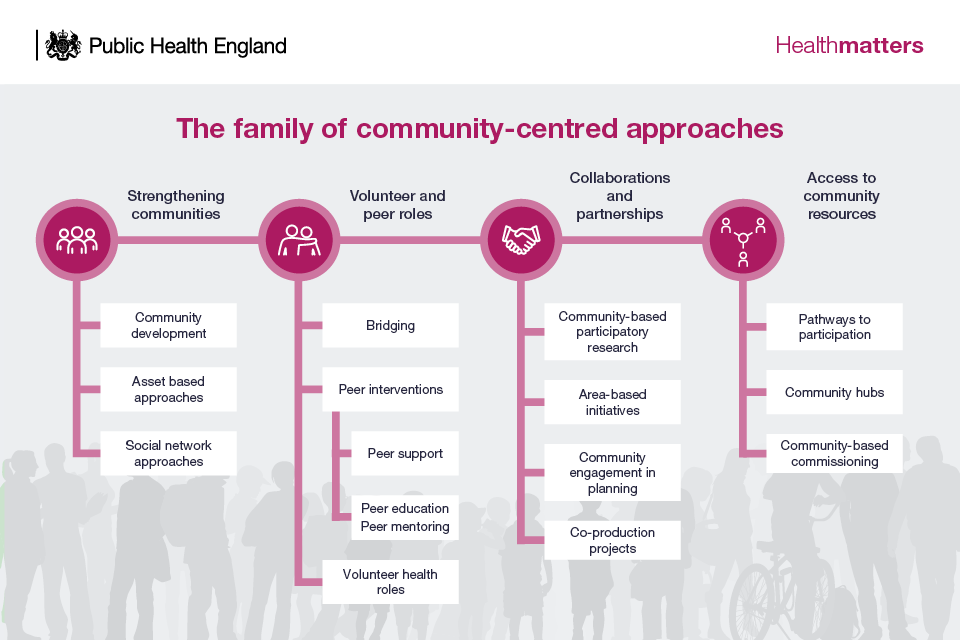
Having scoped the range of approaches and developed an ‘evidence-based framework that could be used in commissioning and practice, in 2015, PHE and NHS England published A guide to community-centred approaches for health and wellbeing introducing the ‘family’ with its four strands:
- strengthening communities
- volunteer and peer roles
- collaborations and partnerships
- and access to community resources (The family of community based approaches illustration (pdf)).
{kind=link}
Health matters: Community-centred approaches for health and wellbeing
‘Community-centred approaches are intrinsically asset-based as they seek to build on the range of informal and formal assets within communities and strengthen the factors that create health. Established asset-based methods that give specific emphasis to mobilising assets are highlighted in the guide, examples include Asset-Based Community Development (ABCD), C2 (Connecting Communities) and time-banking. The intention was for the family to represent a suite of options, not as a technical fix but as a way of translating the goals of improved social connections, greater equity and empowerment into practical action.
‘The work on community-centred approaches moves public health away from thinking about the ‘community’ as merely a setting for services or worse still, a target for professionally determined intervention or change. It is built on an understanding that communities matter for health – aspects such as the quality of social connections, the levels of trust in neighbourhoods, and the confidence to participate are all important determinants of health (Healthy, prosperous lives for all: The European health equity status report).
Conversely, threats to these community-level determinants adversely affect health and widen the health gap through the experience of stress, discrimination, social isolation or loneliness (Psychosocial pathways and health outcomes: Informing action on health inequalities). Developing a community-centred approach in public health means working to maximise the protective factors at a community-level and to mitigate the risks associated with disadvantage. It also means mobilising and strengthening community action and working with people as equal partners (see "What do we mean by community-centred").’
The focus is ‘on the community-level as arguably this has been overlooked in traditional approaches to public health. Of course, a salutogenic approach to health and wellbeing involves much more than interventions with communities. It also shapes the way health is defined and measured which in turn links to an assets model for public health evidence.
While the ‘family’ image serves as a concise reminder of the suite of practical options and the interconnections between community-centred approaches, it aligns with a broader range of asset-based interventions in health and social care. Some of these operate at an individual level or through services and systems. For example, strength-based approaches to managing long term conditions, or recovery methods in social care.’
What do we mean by community-centred?
- Promotes health and wellbeing or reduces health inequalities in a community setting, using non-clinical methods.
- Uses participatory methods where community members are actively involved in design, delivery and evaluation.
- Measure are in place to address barriers to engagement and enable people to play an active part.
- Utilises and builds on the local community assets in developing and delivering the project.
- Develops collaborations and partnerships with individuals and groups at most risk of poor heath.
- There is a focus on changing the conditions that drive poor health alongside individual factors.
- Aims to increase people's control over their lives.
‘The key messages of the PHE and NHS England Guide, Health matters: Community-centred approaches for health and wellbeing, have been incorporated into national strategies and reflected in national public health programmes.
The National Institute for Health and Care Excellence (NICE) Guidance on Community Engagement sets out the principles of engagement for local systems, endorsing the development of long term ‘collaborations and partnerships’ with communities alongside actions to build volunteer and peer roles (Community engagement: Improving health and wellbeing and reducing health inequalities).
Identifying local health assets is a NICE quality standard for community engagement (Community engagement: Improving health and wellbeing quality standard) and NHS England’s recent Universal Personalised Care model recommends that local areas ‘should have in place a range of community-based approaches and a clear understanding of existing community assets and gaps.
While the development of this supportive national infrastructure is important and signals a wider acceptance of community level action, it is public health practice that has really been at the forefront of change.
We have seen a new and growing confidence to use community-centred and asset-based approaches within place-based public health. This means taking action on the wider determinants to improve the areas where people live and work, alongside deep and ongoing partnership work with communities.
Diverse local approaches to improving neighbourhoods and working with communities of interest show how public health commissioners and providers are adapting evidence-based models in local contexts (see chapter two).
PHE now has a suite of practice examples that map to the family of community-centred approaches. Each example, written by local staff, provides a summary of the what, why and how of local programmes and, most critically, the learning that has emerged. There are some fantastic examples of putting asset-based approaches into practice. These include:
- an asset mapping project involving communities in Wakefield
- implementation of a community wide intensive approach to smoking and tobacco control in Hull using an asset-based approach
- an asset-based community development project in housing estates in Weston-super- Mare
- community wellbeing practices that provide an integrated model of community navigation and social prescribing in Halton (PHE Practice Examples - Community-centred and asset-based approaches).
‘There is much to celebrate as community-centred approaches are no longer on the fringes of public health. But we are not there yet in terms of a community-led public health system that values, mobilises and strengthens health assets as part of mainstream policy and action. This vision needs a fundamental shift in the knowledge base, activities and outcomes of public health.
‘Looking forward, what is needed to make that shift?
- Bold leadership that takes a whole system approach to health and wellbeing and fosters collaborations across sectors and with the public and communities.
- Scaling up community-centred approaches and integrating community participation into mainstream public health.
- Workforce development to equip commissioners and practitioners with the skills to mobilise assets and co-produce impactful programmes and services with communities.
- Ensuring the wider workforce and volunteers have the right training and support to develop their capabilities as health promoters in the communities where they live and work.
- Finally, changing what we measure to balance the deficit model of risks and needs with assessment of protective factors and health assets. This must include citizen voice and evidence from those with experience of marginalisation and understanding their stories and solutions to creating health.
‘This is an aspirational list, nonetheless a fundamental shift can be achieved even in difficult times. Fostering community-level change should be an integral part of a whole government and whole-society approach to health. This requires an asset lens and embedding community-centred approaches as the normal way of doing public health.’
2. Implementation and organisational change
In this chapter we look at how the asset-based approach has been implemented, starting with a review of asset-based commissioning taken from the contribution by Janet Harris. We go on to discuss practical examples of implementation drawing on contributions on asset-based work in Scotland, Leeds and Oldham along with case studies throughout this publication from Gateshead, Oldham, Rotherham, Spain and York
Asset-based commissioning is an approach to, ‘Enabling people and communities, together with organisations, to become equal co-commissioners and co-producers, and also via self-help, make best complimentary use of all assets to improve whole life and community outcomes’ (Asset-based commissioning: Better outcomes, better value).
Harris reflects that, ‘ten years ago, ‘A glass half-full’ recommended that commissioning develops approaches to supporting community development and community building, suggesting that asset-based commissioning’ could:
- be aligned with initiatives focusing on place-shaping and wellbeing
- support population-level involvement, which means not only in the process of commissioning but also in deciding what activities are commissioned
- foster co-production of health care with third sector organisations and users
- consider how to invest in long term outcomes and quantify impact’.
Since then, Harris argues, various policies in health, social care and community development have promoted these proposed changes with variable success. ‘When viewed on a continuum, commissioning should be shifting from services based on organisational assets to services based on community and people assets, we continue to be challenged to co-design, co-deliver and co-evaluate services with communities (Engaging and empowering communities: our shared commitment and call to action).
‘There are indications that commissioners are ‘asset aware’, able to draw upon the assets of people and communities to improve or modify an existing service (Asset-based commissioning: Better outcomes, better value). But in some areas a top-down approach that uses statutory services as the starting point is still being taken, which embodies a consultative rather than co-produced approach (The Assets Based Area).
A step change is required where services are re-engineered in response to what is already available in communities – while maintaining an ongoing alignment as new assets are identified to ensure that services compliment what is there and being developed.’
Harris cites the Department for Communities and Local Government (DCLG) which ‘believes there is a consensus on the common barriers to asset-based commissioning, which include:
- a short-term focus
- siloed working
- inability to leverage additional funding
- a top-down approach
- transactional decision making’ (By deeds and their results: How we will strengthen our communities and nation).
These barriers have been ‘consistently identified across national evaluations of integrated health and social care. Short-term funding cycles for completion of specific projects limit the ability to develop longer term partnerships across voluntary and statutory sectors, which is further hindered by a tradition of working in silos within sectors. Although the integration of health and social care has successfully promoted more cross-sector working, progress on integration of budgets has been slow’.
(Early evaluation of the integrated care and support pioneers programme (pdf)), (Developing new care models through NHS vanguards). Harris goes on to argue that fundamental changes are needed in the current commissioning model to move it away from organising along professional specialisms towards a truly people-centred approach. She gives examples of where this is beginning to happen:
- Doncaster Council has established an integrated commissioning plan, working with local communities via integrated neighbourhood teams and assets-based community development to coordinate access to health and social care (Doncaster Health and Social Care Commissioning Strategy 2019-2021 (pdf))
- Kent County Council has established partnering agreements and a strategic partner network, where activities are identified by stakeholders and commissioned using a social value framework (Revitalising the evidence base for public health: An asset model. In Promotion and Education).
Harris identifies ‘five steps commissioners can take to be more asset-based:
- Shift your focus – move your thinking from only considering services as assets to a place-based lens that aims to shape and build people’s, and communities’ assets as well, including the voluntary, community and social enterprise (VCSE) sector.
- Recognise contributions of people – rather than seeing organisations as the only producers of outcomes recognise that outcomes are achieved by people, communities and organisations together.
- Share the decision-making – rather than organisations consulting people and communities before making decisions; make sure people and communities are equal decision-makers from the start and throughout, with investment in community groups to help this process.
- Develop relationships – rather than keeping organisational suppliers at arms’-length, commissioners should ensure greater collaboration with organisations and view VCSE bodies as co-commissioners.
- Commissioning processes – rather than being mostly centralised devolve commissioning to the lowest practical scale, enabling neighbourhood level decision-making (Asset-based commissioning: Better outcomes, better value).
Asset-based commissioning sets the framework for asset-based approaches being adopted in practice. South and Stansfield argue that, ‘looking back since the publication of ‘A glass half-full, the use of community-centred approaches to improve the health and wellbeing of individuals and communities has grown considerably.
Mobilising health assets, including working in partnership with local voluntary and community organisations and volunteers, is very much part of the public health offer for many local authorities’. They go on to describe how PHE now has a suite of practice examples that map to the family of community-centred approaches. Each example, written by local staff, provides a summary of the what, why and how of local programmes, and most critically, the learning that has emerged.
Further examples are described in contributions to this review by Jennifer McLean, Lisa Keenan and Mick Ward, Carolyn Wilkins, and Viola Cassetti.
McLean provides an overview of progress in Scotland arguing that, although there is still a long way to go, asset-based approaches ‘are now firmly located in Scotland’s policy and legislative ambitions for the future (Scottish Parliament, 2010, 2014, 2015)’.
McLean and her team conducted research across a range of settings and ‘found asset-based approaches to be largely practice-based, experiential and sometimes instinctive, a relationship-based way of working which appreciates the connections, contributions and participation of people’. She says that ‘…in Scotland considerable progress has been made, reflective of the supportive and receptive policy landscape, to support community-led action, opportunities for participation, citizen involvement in decision making and a significant move towards more community-based services.
A number of examples of large-scale community-led initiatives and programmes (Knowledge is Power, East Ayrshire Council Vibrant Communities, Inspiring Scotland Link Up programme, Corra Foundation People in Places Programme) are now evident. Supported by funding from national and local government, community groups and organisations from across Scotland have taken and continue to take action on issues that are important to them and which is leading to positive change in and for that community’.
Wilkins, reflecting on her experience in Oldham, describes how ‘the principles and values of strength-based working shape everything that we are trying to achieve. It is not an approach we simply select for certain projects. It is a fundamental shift in how we think about what we do, and how we design and deliver services and support’. In other words, real organisational change. She goes on to say that ‘in Oldham, we believe our starting point should always be developing a deep understanding of the current reality – for communities and local places, but also for organisations and the systems they operate in.
All too often, programs and services are developed in ways divorced from such knowledge. What assets there are, but also how they are seen and understood, can vary dramatically with different perspectives. For example, a park may be seen as a valued space well used by local people.
A different park (or even the same park at different times of the day) might be seen as a place to be avoided. Knowledge of less tangible assets such as social connectedness, levels of trust and distrust, is also crucial. The desire to develop and deepen our understanding is behind the work to build Oldham’s Thriving Communities Index. This maps local assets alongside numerous different data sets, and is on the constant review, ensuring we are continually evolving what we understand about our places and communities’.
One example of the asset-based approach taken in Oldham is their social prescribing programme, which aims to connect people to local assets. It relies on close partnership working. In another example Cassetti describes the network of partnerships at different levels which has been established in Spain as a crucial element of an asset-based approach.
But, Wilkins argues, the learning from places like Oldham is not always transferable – ‘the factors critical to success are often hard to capture in formal evaluations or case study write ups. Therefore, as indicated in ‘A glass half-full’, specific local solutions that come out of asset-based approaches may not be transferable without change. They rely on community knowledge, engagement and commitment which are rooted in very specific local circumstances’.
The Leeds’ approach described by Keenan and Ward was ‘first trialled in three Neighbourhood Networks in Leeds back in 2013/15. This was using what we would now call the ‘ABCD framework’: establishing a Community Builder in the neighbourhood, who identified, enthused and supported community connectors, provided some ‘small sparks’ funding and developed community led and owned asset maps.
While there were challenges, we were confident we could build on the success of these trials, and establish three new ABCD sites, known locally as ‘ABCD pathfinders’ in 2017. The achievements of these pathfinders far exceeded expectations and have shown the transformative potential of people coming together to make changes. We used evidence from the sites to make the case for further funding, importantly this included a contribution from NHS partners, to establish eight more pathfinders in neighbourhoods across the city in 2019’.
An important part of the Leeds approach has been ‘working with providers to see how they can use asset-based approaches within their organisation. This recognises that a service will have a clear remit to deliver on (one unlikely to have been decided by the community), but can still use the principles of connecting people around their interests and seeing the strengths of the people they support. This presents a great opportunity to work with a huge range of organisations in to move towards a more asset-based approach in their day to day work’.
Keenan and Ward conclude that ‘to make a significant shift towards an asset-based approach requires three things: a framework to deliver ABCD; the use of ‘asset-based approaches’ across a wide range of agencies; and that asset-based values are embedded, nurtured and celebrated within individuals, teams and organisations’. Trying to make this organisational shift is not without its challenges. These are explored in chapter three.
There are many more examples from across the country that could have been cited in this chapter. As Wilkins argues ‘There is much to learn from elsewhere. But learning doesn’t mean a simple ‘lift and drop.’ This would risk missing those crucial success factors that meant the change could and did take place. Learning also comes from doing.
It comes from the effort and commitment needed to develop understanding from the work to deepen and improve connections in the building of trust. Working in this way is also about harnessing the power of the unexpected – the alchemy that happens when we commit to principles and values, deeply entwined throughout our own contexts, experiences, ideas and our own rich array of strengths’.
3. Challenges and critiques
In this chapter we focus on critiques of asset-based approaches based on contributions by Shelina Visram, Stephen Crossley and Jennie Popay and summarise the challenges faced by those trying to put asset-based approaches into practice, drawing on Jane South and Jude Stansfield, and Lisa Keenan and Mick Ward in particular.
A key criticism of the asset-based approach is that it fails to address issues of power and that, particularly in a time of austerity, it could exacerbate growing economic and social inequalities. Popay argues that many ‘local strength-based initiatives’, ‘have replaced the problems of the deficit approaches with different but equally significant problems that are by, but not the result of, draconian cuts in public expenditure resulting from austerity’.
As communities are ‘burdened with primary responsibility to address the problems generated by growing social inequalities strength-based approaches are helping create a new world of DIY welfare at the community level, feeding into/supporting the sustained attack on the provision of publicly funded and provided health, social and welfare service[s]’.
She cites a recent Scottish study, Tackling health inequalities through asset-based approaches, co-production and empowerment, where ‘local practitioners admitted that asset-based approaches were often not experienced as empowering by the communities involved and did not contribute to greater social and health equity’. She argues that ‘given the difficult conditions austerity has created for local government in the UK, particularly in more disadvantaged areas, these findings are not surprising’.
Popay goes on to develop a compelling argument that ‘these approaches have strengthened the ‘inward gaze’ on changes in community psychosocial dynamics, individual behaviours and proximal conditions in neighbourhoods. Obviously, professional input should support communities with relatively little power to release or develop the capabilities communities need to take control of local decisions and actions to improve health and wellbeing.
However, as this inward gaze has strengthened, the outward gaze on social transformation and political change for greater health equity, central to foundational statements on community empowerment in the Ottawa Charter, has weakened” (Popay et. al. forthcoming)’.
She points as exemplars the many local health promotion projects adopting an asset-based approach to individual behaviour and lifestyle change, which Friedli argues too often ‘attempt to reproduce in poorer communities, psycho-social assets that are in fact tied to material advantage, while leaving power and privilege intact’. (Reasons to be cheerful: The count your assets approach to public health; What we’ve tried, hasn’t worked’: The politics of assets based public health)
Popay goes on to argue that ‘there are many differences in the lived experience of groups bearing the brunt of social injustice, but it is inequities in power that generate and sustain these inequities and regardless of the context, similar strategies are required to change these dynamics’.’
She maintains that ‘in the UK and elsewhere there are thousands of local ‘asset-based’ community projects supported by front line practitioners and local agencies that highlight community strengths. Whilst purporting to be ‘empowering’’ she suggests that ‘they are local and inward looking and fail to address the fundamental determinants of social and health inequities.’
Finally, she argues that ‘only by mapping the power dynamics that create and sustain the adverse conditions responsible for growing health inequalities and explicitly designing and implementing strategies to support communities to challenge these dynamics at multiple levels – local, regional and national – will these initiatives be operating according to the foundational values and principles of community empowerment for health’. Popay presents two frameworks to aid communities to understand and challenge power.
Visram and Crossley also discuss the importance of power, with a focus on social capital, a concept they see as closely aligned to assets, arguing that ‘there is often little consideration of power or politics in discussions on social capital and asset-based approaches, or of the fact that not all assets are equal in value.
For example, membership of the infamous Bullingdon Club confers a wider range of benefits than those experienced by members of the social clubs and working men’s clubs that are a feature of many UK towns. The literature on asset-based approaches tends to emphasise the importance of psychosocial rather than economic assets, which are rarely mentioned, neglecting the fact that the two are often closely linked. Bourdieu 31, on the other hand, suggests that economic capital is generally required to exchange or convert into cultural and social capital.
‘Time free from economic necessity’ allows people the opportunity to invest in and prolong their education and improve their health, whilst social capital is viewed as a long-term strategy of accumulation that requires effort and energy – it is not a ‘natural given’. Social capital and asset-based approaches can therefore, as Bourdieu argued, contribute to sustaining rather than reducing inequalities, which is arguably how these approaches have been deployed over the last decade’.
They point out that ‘programmes of austerity in Europe and the UK have impacted most on those already vulnerable, such as those with precarious employment or housing, or with existing health problems [and is] associated with worsening mental health and, as a consequence, increasing suicides’ (The Body Economic: Why austerity kills: recessions, budget battles, and the politics of life and death).
They go on to say that the ‘prevailing narrative of people living in poverty and experiencing inequality frames them as shirkers, scroungers or ‘troubled’: a general drain on resources and burden on ‘the taxpayer’, rather than people having assets and resources that are of value (In Their Place: The Imagined Geographies of Poverty). In this context the government has co-opted the asset-based way of working as a way to reduce ‘unaffordable demand’ on services, linked to public spending cuts’.
They conclude that ‘while the goal may be to achieve a better balance between service delivery and community building, this has not yet been achieved in the UK at least. If asset-based approaches are, in part, a reaction to the original welfare state view of citizens as passive recipients of welfare services, then the current context, where people requiring support from the state are portrayed as a burden on the rest of ‘us’, does not provide particularly fertile ground for these views.
Many government policies implemented over the last ten years have led to severe cuts to public services and actively worked against community building efforts. There are examples of local authorities successfully implementing asset-based approaches in the context of austerity, but little evidence that they have had any impact on health inequalities to date. If we want to build on the strengths of local people to improve the health of the communities in which they live, we need to ensure they have a strong economic foundation to engage with programmes that are supposed to help them’.
South and Stansfield concur that ‘as uptake of community-centred approaches increases, the drivers of change are not all positive. Financial constraints have undoubtedly led to local authorities exploring different approaches to using scare resources. Community infrastructure has often faced a reduction in funds. More critically, the impact of austerity has been felt in the poorest communities most (Visit to the United Kingdom of Great Britain and Northern Ireland: Report of the Special Rapporteur on extreme poverty and human rights) and the health inequalities gap is now widening (Health inequalities: Place-based approaches to reduce inequalities).
This does not create easy conditions for implementation of a community-centred approach, and investment in workforce development and community capacity building is needed to do this work well’. But they say that ‘despite these challenges, a place-based approach to reducing health inequalities remains a core strategy in public health.37 We are seeing some local authorities lead transformative change to work alongside local communities to develop better solutions.
For example, Dudley’s work on community resilience which builds action bottom-up starting with local conversations or Wirral’s focus on regeneration of place alongside regeneration of communities (PHE Practice Examples - Community-centred and asset-based approaches) These exemplars of whole system community-centred approaches offer a template for how aspirations to build healthier, more connected and empowered communities can be translated to meaningful action by local leaders’.
In chapter two we outlined several further examples of where local authorities are doing positive work using an assets-based approach. Some contributors are particularly clear about the challenges this can present. For example Keenan and Ward talk candidly about not having been able to scale up their asset-based approach, even though it has shown some success at neighbourhood level: ‘despite our clear focus on prevention and keeping people well, over-stretched budgets are still heavily tipped towards service based solutions‘.
They argue that sometimes it is only possible to go part way towards embodying an asset-based approach through, for example ‘working with providers to see how they can use asset-based approaches within their organisation. This recognises that a service will have a clear remit to deliver on, one unlikely to have been decided by the community, but that can still use the principles of connecting people around their interests and seeing the strengths of the people they support’.
Keenan and Ward identify four major challenges that they have faced in promoting an asset-based approach at a local level:
- 1. We already do that: ‘If we are truly to work in asset-based ways across health and social care and beyond, then we need to redefine our relationships with communities. It is understandable then, that people and organisations may feel reluctant to make these significant changes. Some organisations when discussing asset-based approaches claim to be doing so already, and therefore do not need to change. And, whilst they are often doing some very good work, it is not often asset-based.’
- 2. Making it work for all: ‘we recognise that these communities may not always be inclusive for all. This is particularly relevant for adults and health in terms of those with care and support needs.’ They cite, for example, those with learning disabilities.
- 3. The importance of continuing to fund existing services – ie not using an asset-based approach as an excuse for cutting back on direct service provision, a danger emphasised by other contributors.
- 4. Traditional evaluation and reporting – which is deficit based. Keenan and Ward argue that there needs to be a different approach to assessing outcomes in an asset-based approach. ‘It is not about simply counting numbers of people who show up, but about nurturing and celebrating participation and contributions that strengthen community life, providing those connections that we know are so valuable.’
Cassetti identifies further challenges in a key aspect of asset-based approaches – partnership working. She argues that ‘boundaries (visible and invisible) between agencies tend to persist, making intersectoral work a challenge for many’. She identifies common challenges across many countries where governmental structures ‘tend to work in silos, lacking support and policies which could enable a more intersectoral approach to thrive’. She also highlights the tendency for partnerships agreed at governmental or local authority (horizontal) level not to be replicated between different parts of organisations (vertical) which continue to work in their usual siloed way.
In addition, she argues that, ‘although having a shared mission has been found to be central in any partnership, there are other factors which can enable or hinder intersectoral work, such as having time to dedicate to the partnership and to the establishment of trustworthy relationships, good communication between members, and the adoption of inclusive and participatory approaches’ (Promoting intersectoral and interagency action for health and well-being in the WHO European Region).
And along with Keenan and Ward, she also identifies evaluation as a challenge for partnership working.
Keenan and Ward conclude that ‘changing attitudes, values and culture (in local government) can be challenging and takes a long time. Even ten years after the publication of ‘A glass half-full’, there is still much to do. We (politicians and officers) may not yet be changed, but the journey is changing us. We’re just at the beginning of re-imagining how services and support could look if we are to truly support communities to come together, connect and take the lead’.
In conclusion it remains important to continue to take a critical perspective on asset-based approaches and to recognise their limitations. Asset-based approaches can undoubtedly be used as a cover for handing responsibility for addressing health and social inequities to disadvantaged communities, whilst cutting back on the infrastructure and economic factors that are the root causes of inequities. Questioning and challenging power dynamics remains crucial. Those adopting an asset-based approach need to be continually reflective and recognise the challenges inherent in remaining true to the central value of community control.
4. Leadership
Councils have faced huge financial challenges over the past decade and these show no signs of ending. Demand for services is rising while austerity has led to drastic cuts in their income. According to the LGA: ‘by 2020, local authorities will have faced a reduction to core funding from the Government of nearly £16 billion over the preceding decade. That means that councils will have lost 60p out of every £1 the Government had provided to spend on local services in the last eight years. Next year [2019] 168 councils will receive no revenue support grant at all.' (Local Government Funding, Moving the Conversation on)
In response to these challenges many councils have sought to build on, or develop, new ways of doing things. One of these has been to adopt an asset-based approach. To achieve this shift and take it beyond the small scale to the transformative, requires culture change, leadership and political commitment.
This chapter draws from all the contributors to this review to argue that this shift needs to be system-wide and built on developing relationships between partners and on a transfer of power within councils and partner organisations and between these and communities. This argument is illustrated by drawing on the contribution by Councillor Keith Cunliffe and Kate Ardern in which they describe how Wigan Council moved, following devolution, to a system-wide approach to addressing the challenges the borough faces. This has building on community assets at its heart.
Traditionally the response a council makes to an emerging priority has been to identify and implement an intervention to address or minimise its impact. According to the National Philanthropy Centre: ‘each time we develop an intervention, we paper over the cracks and layer yet more complexity onto an already complicated and confused system.
The problem with this approach is that the interventions only last as long as there is the political will to support and fund them. There are few examples of such interventions becoming hard-wired into mainstream services or of these addressing the root causes of structural, societal and systemic disadvantage –even from times of plenty' (Systems Change, a Guide to What it is and how to do it).
Taking a whole-systems approach is about seeking to address the root causes of problems and changing how they are tackled in a way that moves beyond the margins into the mainstream. To truly effect change, support for different ways of doing things needs to happen at all levels, from the national to the neighbourhood.
The contribution by Cassetti on the Spanish approach to partnership working illustrates how this was nationally-led and permeated all levels across the system. ‘In Spain, the National Health Promotion and Prevention Strategy, centres around working collaboratively across different sectors and encourages the creation of local health alliances where different sectors come together to plan collaboratively actions to promote health and wellbeing in local areas or municipalities.’
In Scotland an asset-based approach has been led by the National Assembly with support from the Scottish Community Development Association. As McLean states in her contribution this is now ‘firmly located in Scotland’s policy and legislative ambitions for the future’. While there has not been this sort of national support in England areas like Greater Manchester are supporting an asset-based approach across the region. In other places the lead has come from councils as illustrated by the examples from Gateshead, Leeds, Oldham, Wigan and York.
Whether it is at national, regional, district or community level, progress is dependent on effective and innovative leadership at all levels and political support for a transformational shift in how things are done. Local authorities are well placed to take the lead at a regional and district level but to be truly transformative, system change has to happen across partners. This relies on building constructive relationships based on trust. Councils and partner agencies need to work harder to build trust with their communities and demonstrate there has been a genuine transfer of power to individuals, families and citizens that allows them to exercise more control over their lives.
In Greater Manchester devolution has provided opportunities for local determination of how resources are deployed and enabled a more asset-based approach. Cunliffe and Ardern describe how in Wigan the financial challenges they face and the opportunity devolution presented to do things differently, has led to ‘politicians and senior management fundamentally re-thinking how they could create a new relationship with residents and communities’. The outcome has been the development of the Wigan Deal based on the following set of public service reform principles:
- A new relationship between public services and citizens, communities and businesses. Do with, not to.
- An asset-based approach that recognises and builds on the strengths of individuals, families and communities rather than focusing on the deficits. Having a ‘blank mind’ when having conversations. Treat citizens as full of strengths to be revealed.
- Behaviour change in our communities that builds independence and supports residents to be in control.
- A place-based approach that redefines services and places individuals, families, communities at the heart. Stay close to neighbourhoods and mobilise people around them.
- A stronger prioritisation of wellbeing, prevention and early intervention.
- An evidence-led understanding of risk and impact to ensure the right intervention at the right time.
The Wigan Deal has led to significant improvements in public health outcomes and importantly has proved popular with residents. Staff are central to this success, including appointing the right staff to support transformation, two of the most important attributes being energy and motivation for change. Innovation is key to progress and staff must be given the time and space to try new things, to make mistakes at times and learn from them. Wigan has developed a culture of ‘giving good people the time and space to do great things. Evidence-based working is important, but evidence can only be achieved in the first place by trying something new’
Ardern in her blog, Bottom-up working for effective place-based leadership, on the NHS Confederation website says: ‘new staff are recruited to core characteristics of being positive, courageous and accountable... for more longer serving staff, we have needed to understand better how the culture of organisations can discourage innovation and staff using their own judgement.
This means that sometimes we have to help colleagues unlearn some work behaviours and, in many cases, staff feel empowered and know they have permission to act. We encourage staff to learn new approaches, to hold asset-based conversations wherever they go, and to use their own judgement to make quick decisions in line with agreed guidelines. There are many fantastic examples of the difference this has made to citizens’ health and wellbeing and the morale and motivation of staff… Rediscovering their vocation is a common theme’
One challenge for staff has been building trust in communities that have seen new initiatives come and go. People have been told they would be listened to and changes made, only to have the same old services delivered time and again. Allowing staff time to work with communities and build relationships and trust has been key. Wigan has also learnt that, while it was often useful to work with established community leaders, they had to work hard to engage marginalised communities that might not be represented by those leaders
For any council seeking to build relationships and trust with communities, it will be crucial to have long-term, open-ended funding for community development which frees staff, including those in voluntary sector organisations, to engage with communities independent of commissioned outputs.
Not only is the local voluntary sector an ideal conduit through which community action can be fostered, but also in many places there are established ‘community hubs’ or anchor organisations that are located in neighbourhoods and have been present there for long periods and are familiar to local people (Building healthier communities: the role of the NHS as an anchor institution). Cassetti describes:
‘An increasing phenomenon in the US which has started to generate interest in Europe is that of anchor institutions to tackle the intermediate and wider health determinants. Anchor institutions are institutions with financial capital who are ‘anchored’ in communities, ie they are not likely to go away if a crisis come or market trends change.
They are generally non-profit organisations, mainly public (such as hospitals, health centres, universities) and are place-based. Anchor institutions can therefore establish policies to employ locally, source locally, build locally and work collaboratively in partnerships for (ideally) long term, thus favouring the sustainability of local health initiatives. They can become an important asset in the fight to reduce health inequalities as they can become ‘drivers of economic development.’
As noted above, leadership both at a political and organisational level, is critical to success in embedding asset-based approaches. A ‘dispersed’ leadership style is best suited to this approach freeing others up to build direction, purpose, a new relational culture and in fostering reciprocal partnerships and collaborations. As Ardern notes in her blog:
‘This way of working requires a different set of management styles than we sometimes are used to in the NHS, and the difference in management culture is one that NHS place-based leaders really need to understand and embrace. In local government, the officer code of conduct helps to set some ways of working and standards of behaviour for our leaders and the Wigan Deal takes these guidelines for public service even further.
Compare that (NHS management style) to our bottom up, empowered approach where we prefer continuous improvement and a culture where staff are monitored less and encouraged to challenge themselves to improve the way that they work It’s a very different approach and one we feel is working for people in Wigan.’
Those leading asset-based approaches need to understand to process involved. Attempts to illustrate the stages of development that are needed when adopting asset-based practice at an organisational and system level through the use of a Theory of Change (ToC) could be useful. An example is given in Head, Heart and Hands: Asset based approaches in health care and clearly illustrates the cultural change needed.
Theory of change
Reframing thinking, goals and outcomes Exposure to underpinning ideas, reassessment of current practice and priorities towards asset-based working and the identification of champions to drive change
Recognising the assets available to achieve the change Mapping and describing the individual, organisational, associational, economic, cultural and physical resources available to communities
Mobilising the assets for a specific purpose Understanding and agreeing how community assets can be connected and used. New relationships, new approaches to leadership, systemic action across organisational boundaries
Co-producing outcomes On the pathway to the long-term goal. Co-production of services and outcomes by professionals and citizens. The coming together of equals, each with assets and strengths, around a common goal or a joint venture
Head, Heart and Hands: Asset based approaches in health care
Critical to the cultural change needed is the need to let go of power. Ardern comments: ‘As leaders, we empower staff. As organisations working in Wigan, we seek to nurture citizens’ experience and talents celebrating their good ideas and helping make good things happen. We are happy to ‘lose control’, and that philosophy is an important one to reflect on.’
The journey to achieving positive outcomes in Wigan has not always been smooth and the challenges for health improvement remain great but as Ardern says ‘we don’t learn without acting, and we don’t learn without making mistakes. We are constantly reflecting on what we do and supporting an environment of continuous improvement.’
The real innovation challenge is not about having the ideas, but working out how to turn those ideas into action. We’ve cited many great examples in this publication, but that journey is still all too rare in the public sector. It requires resilience, leadership, risk–taking, effective decision making and has to work across systems.
The recent publication from PHE is clear that ‘Local public health leaders are in a strong position to scale up community-centred approaches across local systems. Effective place-based working across sectors and in partnership with communities can improve health outcomes and meet other local priorities’ and that taking a whole systems approach to tackling the wider determinants and supporting community approaches. Hence ‘Building healthy, resilient, connected and empowered communities is a public health priority shared across many sectors.
A whole system response is needed to maximise impact and improve the health of the poorest fastest. This involves scaling a range of community-centred approaches, addressing community level determinants and working at all levels of a system’ (Community-centred public health: Taking a whole system approach).
As Wilkins, reflecting on her experience in Oldham, says, ‘the principles and values of strength-based working shape everything that we are trying to achieve. It is not an approach we simply select for certain projects. It is a fundamental shift in how we think about what we do, and how we design and deliver services and support’
What the Wigan deal and our other practice examples exemplify is the importance of clarity of political purpose; having ambition and working to scale; and of leadership – both at the top to drive the vision forward but very importantly at all levels so that staff are enabled to work differently and citizens feel empowered to get involved.
None of this is easy in financially challenging times and an asset-based approach should not be seen as a replacement for properly funded services which are adequate to meet needs and address inequalities. Asset-based approaches do however offer a way of achieving much greater engagement and real power sharing across diverse communities.
Postscript by Jane Foot
“My speculation is that the same set of influences that led to England and the UK looking unhealthy in the decade after 2010 led to us having the worst excess mortality figures in Europe because of COVID-19. Such speculation can be given substance if we look at the coronavirus inequalities.
Here we find that there is once again a social gradient in mortality rates from COVID-19 – the more deprived the area, the higher the number of deaths. This social gradient is almost exactly paralleled by the social gradient for all causes of death. It suggests that the causes of unequal COVID-19 outcomes are rather similar to the causes of inequalities in health more generally.”
“The coronavirus pandemic has brought immense pain and hardship to people across the world. But alongside this pain we have also witnessed the extraordinary response of our communities: from the kindness and compassion of neighbours helping neighbours, to the community organisation staff and volunteers who have been working day-in day-out, alongside other key workers, to help get people through the hardest of times…the collective endeavour of emergency support has strengthened partnerships between local government and community organisations. Historical inter-organisational friction engendered by competitive tendering and funding has become irrelevant. Previous siloes and barriers were sidestepped, and trust-based collaboration formed in their place.
We were built for this” (Locality 2020) Mark Law, Chair Locality.
The COVID crisis has been heart-breaking and frightening for all of us. As many of our contributors have said, lockdown has made visible the inequalities in our living conditions and in our health, which Marmot highlighted in 2010 (Health Equity in England: The Marmot Review 10 Years On). The weaknesses in our public services and our care system have been exposed. Mental health and mental health services are both fragile and overstretched.
However, what has also been made visible are the capacities and strengths of many communities and local areas, the necessity and potential of collaboration, and the need to rethink how we value and deliver care to those who need support to live fulfilling lives. Our focus has to shift to what creates health for people and communities.
People and Places matter to our health and wellbeing
Since we published A glass half-full in 2010, the fundamental asset principle that we should value the “capacities, skills, knowledge, connections and potential in a community” and design our public health and community development interventions accordingly has been taken on board by many practitioners; this publication is witness to that.
We can now be more confident in our basic proposition. Strong community networks, neighbourliness and friendship; the benefits of working together and a belief in our own resources have led to and sustained the explosion of mutual aid groups during lockdown.
Without this support many families and older people would have had a much harder time. Foodbanks, good neighbour schemes, delivering prescriptions and walking the dog have become important lifelines for many – both for those who volunteer and for those who have benefited (who are sometimes the same people of course).
Where I live, all the local groups and activities: sports clubs, musicians, bonfire societies, Morris dancers, residents’ groups, faith groups, political groups, cyclists, dance and arts networks and many more -have volunteered to help with a massive food collecting operation that has not only kept people in food but built the solidarity that we will need in the future.
In some areas, there was an existing social infrastructure of resources and relationships already on the ground and active, in some areas it was dormant or fragmented. We have seen the value of connections and understanding between communities and local services, and the importance of building up that trust and collaboration.
Collaboration and co-production is both possible and necessary for local resilience
Centralised and stand-alone solutions have not worked, cut off as they are from the skills and knowledge held locally. Putting our trust in local solutions, delivered in partnership and grounded in existing relationships with local people and sector agencies has been more effective.
We have learnt that it is possible and necessary to collaborate. Joined up working has been achieved where it was hard to imagine. The invention of new ways of working has been accelerated. Local government including public health, health and care services and civil society have come together, pooling their assets and resources of time and knowledge and much more.
Commissioning policy and practice now needs to follow this learning, with a move away from transactional and inflexible service models to develop place based commissioning of public sector services. This needs to include a focus on growing local social enterprise and social value (The community paradigm: Why public services need radical change and how it can be achieved). Services should be brought back in-house and enabled to be more innovative and responsive to local circumstances.
There is evidence that pandemic experience has created some resilience as South et al say. The test will be whether we can sustain that resilience and whether we can go on to transform public health service and invest in measures that will counter health inequalities and promote wellbeing (Health matters: Community-centred approaches for health and wellbeing, The social determinants of health and the role of local government).
The role of local publicly funded agencies is to collaborate with communities and nurture their capacity to act together. But it is also to deliver those things that communities cannot deliver and which are so crucial to health and wellbeing. As we emphasised in A glass half-full (2010) “the asset-based approach does not replace investment in services or tackling the structural causes of inequality”.
This is still true and urgent. As this crisis goes on, inequalities are deepening. How do we support people sheltering from or recovering from COVID-19, the continuing crises of mental fragility, economic hardship, food and fuel poverty, isolation and loss? As well the already increasing gap in mortality, there is a growing visibility and concern for those living with life limiting conditions and chronic illnesses that make them vulnerable not just to COVID-19 but also to other hardships. The need for us to collaborate is more urgent. But so is the duty to act to reduce the inequalities baked into our housing, education and employment structures.
Care is more than residential homes and domiciliary care
If we have learnt anything, it is that we need to invest massively in our care system and in the staff who work in those settings. But we have also learnt that the capacity to care is an underappreciated resource in our neighbourhoods and networks.
As we finally take on, confront and recognise the necessity to think about how we care for our neighbours and families we must challenge our attitudes and priorities. Care and a caring community must be prioritised: those who care for children, those with conditions that limit their lives, those that are elderly as well as those that provide the emotional and physical care. While we ‘build back better’ to cope with the climate emergency; we also need a social recovery to parallel the green recovery. These are linked through the notion of caring for each other and for future generations.
This moment can be an opportunity to rethink our attitudes to caring and work on ways to create a more caring society that recognises both our interdependence and our vulnerabilities. The conversations about a ‘national care service’ should be based firmly in asset principles, nurturing the strengths and networks in families and communities, and enabling those that need care services to remain connected to and to participate in the everyday life around them.
Acknowledgements
The project team Trevor Hopkins, Simon Rippon and Judy White would like to thank the project team at the Local Government Association (LGA), Mark Norris, Paul Ogden and Katerina Charalambous for their help, input and advice throughout the study. Also Kate Ardern, Viola Cassetti, Stephen Crossley, Keith Cunliffe, Jane Foot, Janet Harris, Lisa Keenan, Jennifer McLean, Bengt Lindstrom, Antony Morgan, Jennie Popay, Jane South, Jude Stansfield, Shelina Visram, Mick Ward, Carolyn Wilkins and Erio Ziglio for their valuable contributions and input to this report.
Disclaimer
The views in this report are the authors’ own and do not necessarily reflect those of the Local Government Association (LGA). For more information about the LGA’s Research and Information team.
References
1. Foot, J., Hopkins, T. (2010) A glass half full: How an asset approach can improve community health and well-being. I&DeA/ LGA.
2. Morgan, A., Ziglio, E., (2007) Revitalising the evidence base for public health: An asset model. In Promotion and Education. Supp 2
3. Marmot, M., et al (2010) Fair Society, Healthy Lives – The Marmot Review.
4. Closing the Gap in a Generation Health equity through action on the social determinants of health. WHO Global Commission on Social Determinants. (2008)
5. Ottowa Charter for Health Promotion (1986) World Health Organization
6. Charting the Way to Wellbeing (2012) World Health Organization
7. Due North - Report of the Inquiry on Health Equity for the North (2014) University of Liverpool and Centre for Local Economic Strategies
8. Health matters: Community-centred approaches for health and wellbeing (2018) Public Health England
9. Healthy, prosperous lives for all: The European health equity status report (2019) World Health Organization Regional Office for Europe
10. Psychosocial pathways and health outcomes: Informing action on health inequalities (2017) Public Health England/ University College London – Institute of Equity
11. Morgan, A. (2014) Revisiting the Asset Model: A clarification of ideas and terms. Global Health Promotion, 21(3): p. 2-6.
12. Engaging and empowering communities: our shared commitment and call to action (2016) Think Local Act Personal
13. Community engagement: Improving health and wellbeing and reducing health inequalities – NICE guideline NG 44. (2016) National Institute for Health and Care Excellence.
14. Community engagement: Improving health and wellbeing quality standard [QS148] (2017) National Institute for Health and Care Excellence. [cited 2019 30th September]
15. Universal Personalised Care (2019) NHS England
16. PHE Practice Examples - Community-centred and asset-based approaches (undated) Public Health England [cited 2019 30th September]
17. Field, R., Miller, C. (2017) Asset-based commissioning: Better outcomes, better value – Bournemouth University.
18. The Assets Based Area. TLAP.
19. By deeds and their results: How we will strengthen our communities and nation (2019)
20. Erens, B., Wistow, G., Mounier-Jack, S., Douglas, N., Jones, L., Manacorda, T., & Mays, N. (2016). Early evaluation of the integrated care and support pioneers programme (pdf)
21. Developing new care models through NHS vanguards (2018) National Audit Commission
22. Doncaster Health and Social Care Commissioning Strategy 2019-2021 (pdf)
23. Service specification for the purchase of Community Mental Health and Wellbeing (2018) Kent County Council
25. East Ayrshire Council Vibrant Communities
26. Inspiring Scotland Link Up programme
27. Corra Foundation People in Places Programme
28. de Andrade, M. (2016) Tackling health inequalities through asset-based approaches, co-production and empowerment: Ticking consultation boxes or meaningful engagement with diverse, disadvantaged communities? Journal of Poverty and Social Justice, 24:1
29. Friedli, L, (2011). Reasons to be cheerful: The count your assets approach to public health Perspectives Magazine of Scotland’s Democratic Left, 30
30. Friedli, L. (2013). ‘What we’ve tried, hasn’t worked’: The politics of assets based public health. Critical Public Health, 23(2)
31. Bourdieu, P. (1986). The forms of capital. In Richardson JG (ed). Handbook of Theory and Research for the Sociology of Education. New York: Greenwood
32. Stuckler, D., Basu, S. (2013). The Body Economic: Why austerity kills: recessions, budget battles, and the politics of life and death. New York: Basic Books.
33. Crossley, S. (2017). In Their Place: The Imagined Geographies of Poverty. London: Pluto Press.
34. Alston, P. Visit to the United Kingdom of Great Britain and Northern Ireland: Report of the Special Rapporteur on extreme poverty and human rights. A/HRC/41/39/Add.1. 2018, United Nations General Assembly: Geneva.
35. Health inequalities: Place-based approaches to reduce inequalities (2019) [cited 2019 30 September ] Public Health England.
36. Corbin, J. H., Jones, J., & Barry, M. M. (2018) What makes intersectoral partnerships for health promotion work? A review of the international literature. Health Promotion International, 33(1)
37. Promoting intersectoral and interagency action for health and well-being in the WHO European Region: Synergy among the health, education and social sectors (2015) World Health Organization Europe
38. Local Government Funding, Moving the Conversation on (2018) Local Government Association
39. Abercrombie, R., Harries, E., Wharton, R., (2015) Systems Change, a Guide to What it is and how to do it, NPC
40. Bottom-up working for effective place-based leadership, Kate Ardern
41. Reed, S,. Gopfert, A., Wood, S., Allwood, D., Warburton, W., Building healthier communities: the role of the NHS as an anchor institution (2019) The Health Foundation
42. Hopkins, T., Rippon, S., (2015) Head, Heart and Hands: Asset based approaches in health care. The Health Foundation
43. Community-centred public health: Taking a whole system approach – Briefing of research findings (2020) Public Health England
44. Marmot, M., Allen, J., Boyce, T., Goldblatt, P., Morrison, J., (2020) Health Equity in England: The Marmot Review 10 Years On. The Health Foundation
45. Marmot, M. (2017) Dealing with an epidemic of disempowerment – Health Foundation
46. Shaping places for healthier lives
47. Lent, A. Studdert, J. The community paradigm: Why public services need radical change and how it can be achieved (2019) New Local Government Network
48. The social determinants of health and the role of local government (2010) Ed. Campbell, F. Local Government Association
Webinar presentations: 10 December 2020
Authors/editors

Jane Foot was a community worker, a policy officer and an independent researcher and policy consultant.
She was the co-author of ‘A glass half-full: How an asset approach can improve community health and wellbeing’ in 2010 and wrote the follow-up ‘What makes us healthy?’ in 2012.
She is now retired.

Trevor Hopkins is one of a small but growing group in the UK who, since 2007, have been championing the use of asset-based approaches to improve health, resilience and wellbeing outcomes and challenge preventable inequalities for individuals, families and communities.
In 2010 he co-authored the hugely influential and internationally recognised publication ‘A glass half-full: How an asset approach can improve community health and wellbeing’. This brought the concept of asset-based approaches to a much wider audience than the mainly academic researchers and writers who had developed these ideas over the previous 35 years.
Trevor runs ‘Asset Based Consulting’ with his wife Jayne and they are currently working with county, city, borough councils and voluntary and community sector organisations to develop, deliver and evaluate asset-based approaches to improving health, care, resilience and wellbeing services.

Simon Rippon has been involved in a range of initiatives related to promoting mental health, wellbeing and resilience in communities. He has an interest in health assets and participatory approaches to community and organisational development.
He has co-authored a number of publications on asset-based approaches in the UK. His work includes evaluation and research projects on community development for wellbeing and mental health.
Simon works as a consultant with Aligned Consultancy and has a Visiting Research Fellowship at Leeds Beckett University in the School of Health and Community Studies. Simon has worked extensively with local authorities, the NHS and voluntary and community sector on a range of development programmes related to community development, health assets and civic involvement.

Judy White worked in the voluntary and community sector for ten years, then for health promotion in the NHS for over 20 years during which she set up the early adopter Health Trainer programme in Bradford and helped develop health trainers regionally and nationally.
In 2008 Judy joined Leeds Beckett University where she was a Senior Lecturer teaching on the MSc in Health Promotion. In 2012 she set up Health Together with Professor Mark Gamsu and Professor Jane South with the aim of harnessing the power of active citizens to improve health and wellbeing and address inequalities.
Judy retired in 2017 but remains an Associate Lecturer at Leeds Beckett and undertakes freelance research and evaluation whilst being active as a volunteer in community-based health promotion in her home city of Bradford.
Additional contributions from international, national and local practitioners and academics.
Asset-based approaches in local authorities: achieving a better balance between service delivery and community building
Dr Shelina Visram and Dr Stephen Crossley
Asset-based approaches in local authorities: the Leeds experience
Lisa Keenan and Mick Ward
Asset-based approaches in local authorities: the Oldham experience
Dr Carolyn Wilkins OBE
Asset-based approaches in local authorities: the Wigan experience
Cllr Keith Cunliffe and Professor Kate Ardern
Asset-based approaches in practice: the Scottish experience
Dr Jennifer McLean
Asset-based public health: shifting evidence and practice
Jane South and Jude Stansfield
How commissioning is supporting community development and community building
Dr Janet Harris
Power, politics and community assets
Jennie Popay
Resilience as a major asset to improve population health and wellbeing: a summary of studies and international experiences
Emily Hughes Ziglio and Erio Ziglio
Salutogenesis
Professor Bengt Lindstrom MD PhD DrPH
Place-based partnership working
Viola Cassetti