Inequity, the systematic difference in health outcomes of populations due to avoidable antecedent factors, can be reduced by redistributing public resources. One alliance partnership organisation in South East Essex created an evidence-based scoring tool to map how sufficiently their commissioned community projects service the six social determinants of health, outlined in Michael Marmot’s ‘Fair Society Healthy Lives’ report. Commissioned (shortlisted) projects were scored on two measures: alignment and predicted effectiveness. Alignment was assessed by comparing each project summary to Marmot’s “framework of indicators”. Scoring was between 0 to 3 for both measures (0 no alignment/likely no effect, 1 slightly aligned/effective, 2 moderately aligned/effective and 3 very aligned/effective). The method was repeated on non-shortlisted projects.
South East Essex Alliance is a partnership of:
- NHS (Mid & South Essex Integrated Care Board, Mid & South Essex Foundation Trust (the acute hospitals trust), Essex Partnership University Foundation Trust (the mental health trust and community provider)
- Local authorities (Southend Unitary Council, Essex County Council)
- Community and voluntary organisations (Southend Association of Voluntary Services, Castle Point Association of Voluntary Services)
- Healthwatch organisations (Healthwatch Southend and Healthwatch Essex)
The challenge
The South East Essex alliance were given a non-recurrent grant of £922,000 in May 2022 by the local National Health Service Integrated Care Board. The money was to be allocated rapidly to community projects to address health inequity with limited formal guidance on how it should be distributed.
The solution
On reflection it was felt a simple evidence-based scoring tool would have been useful to inform the allocation process. The team investigated whether the six policy areas proposed in Michael Marmot’s ‘Fair Society Healthy Lives’ report,[2] mapped onto the shortlisted and excluded projects objectives, and thus form the bases of such a scoring tool for future use.
Marmot’s six social determinants of health inequity are:
- Give every child the best start in life
- Enable all children, young people and adults to maximise their capabilities and have control over their lives
- Create fair employment and good work for all
- Ensure a healthy standard of living for all
- Create and develop healthy and sustainable places and communities
- Strengthen the role and impact of ill-health prevention
Commissioned (shortlisted) projects were scored on two measures: alignment and effectiveness. Alignment was assessed by comparing each project summary to Marmot’s “framework of indicators”. Scoring was between 0 to 3 for both measures (0 no alignment/likely no effect,1 slightly aligned/effective, 2 moderately aligned/effective and 3 very aligned/effective). The method was repeated on non-shortlisted projects.
The work was conducted at the local authority level: led by two public health doctors working for Essex County Council (Dr Gabrielle Sanders, a junior doctor partaking in a public health rotation for four months, and Dr Danny Showell, public health consultant) and two public health doctors at Southend City Council (Dr Khushbakht Khan, a junior doctor also based in public health for 4 months and Dr Margaret Eni-Olutu, public health consultant).
The local authority public health teams work with other partners in the South East Essex Alliance to identify the needs within the communities of Southend, Castle Point and Rotchford, using data gathered from the local population, and allocate funding to projects within the community which will best address the needs of the population served.
The impact including cost savings/income generated if applicable
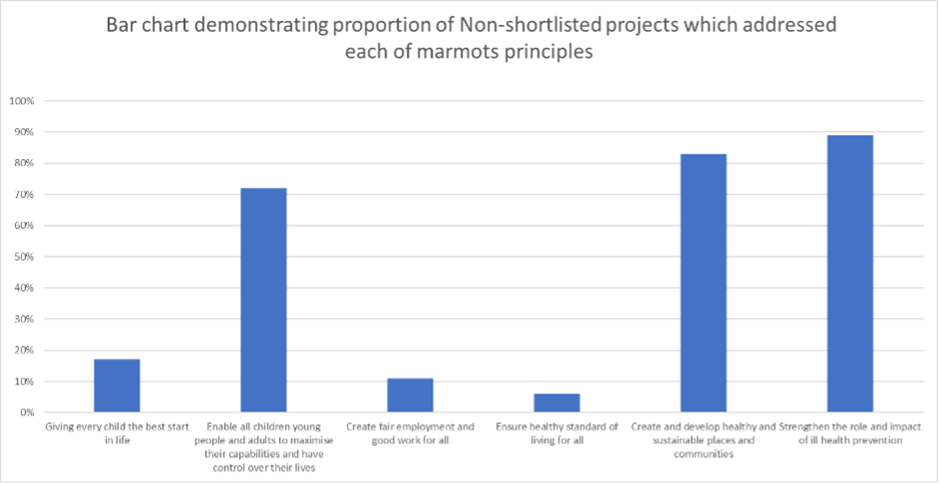
There was a skewed distribution of Marmot principles in shortlisted, and non-shortlisted cohorts. Overall, most projects addressed principles 5 and 6. The least addressed was principle 3 (10 per cent in both), followed by principles 4 (25 per cent in shortlisted; 11 per cent in non-shortlisted), 1 (35 per cent; 17 per cent) and 2 (40 per cent; 72 per cent). The marked difference between the shortlisted and not cohorts in the latter, demonstrates potential for mapping to highlight addressed drivers of health inequity and focus on those unaddressed.
Moreover the grossly under-addressed principles 3 and 4 pose a public health issue, recognised by the World Health Organization and International Labour Organization, [3] especially with the current global backdrop of an increasing cost of living,[4] financial income and the quality of employment will have paramount impact on public health.
The gaps identified in the alliance’s health inequity strategy have subsequently informed the distribution of remaining funds toward the voluntary sector and employment initiatives in the local community.
How is the new approach being sustained?
The team plan to map future project bids to Marmots six social determinants and use this as a starting point to approaching project shortlisting.
The findings have been shared with other alliances within both Essex County Council and Southend City Council to encourage creativity, build on existing knowledge, and encourage evidence-based practice, with the over-arching goal of improving current practice.
Lessons learned
The final scores generated in this mapping process should not be absolute, but a helpful guide.
It is recommended each project is scored by many members, diverse in line of work and values, of the local commissioning board as a group to ensure consensus is reached and discrepancies can be debated.
Several lenses should be applied when selecting projects for funding to address health inequity; a combination of tools is advised to be used in conjunction with one another, such as Core20plus5 and population health management priorities to ensure vulnerable groups are addressed.
Case study submitted by: Dr Gabrielle Sanders, Dr Khushbakht Khan, Dr Daniel Showell, Dr Margaret Eni-Olotu
Contact: [email protected]
Links to relevant documents
[1] Lee H, Kim D, Lee S, Fawcett J. The concepts of health inequality, disparities and equity in the era of population health. Appl Nurs Res. 2020 Dec [Cited 2022 Nov 14];56:151367. Available from: doi: 10.1016/j.apnr.2020.151367. PMID: 33280788.
[2] Marmot M, Allen J, Goldblatt P, Boyce T, McNeish D, Grady M, et al. The Marmot review: Fair society, healthy lives. London: UCL. 2010 Feb. [Cited 2022 Nov 25] Available from: https://www.instituteofhealthequity.org/resources-reports/fair-society-healthy-lives-the-marmot-review
[3] Burton J, World Health Organization. WHO healthy workplace framework and model: background and supporting literature and practices [Internet].Switzerland: World Health Organization [2010; Cited 2022 Nov 14]. Available from: WHO Healthy Workplace Framework and Model
[4] The Lancet Public Health. The cost of living: an avoidable public health crisis. Lancet Public Health. 2022 Jun 01;7(6):e485. doi: 10.1016/S2468-2667(22)00120-7. PMID: 35660204; PMCID: PMC9159733.
Table 1: Template of how scoring was performed with respect to alignment with Marmot’s six principles and predicted effectiveness in fulfilling their aims.
Appendix 1
|
Project Summary |
Principle 1 |
Principle 2 |
Principle 3 |
Principle 4 |
Principle 5 |
Principle 6 |
Total |
|
A |
Alignment = 2 Effectiveness= 3 |
1 2 |
0 0 |
3 3 |
3 2 |
3 3 |
Total alignment= Av. Effectiveness= |
|
B |
1 0 |
3 2 |
0 0 |
2 3 |
2 3 |
2 2 |
|
|
C |
0 0 |
1 3 |
2 3 |
3 2 |
1 3 |
3 3 |
|
|
Sum of projects aligning with each principle |
2 |
3 |
1 |
3 |
3 |
3 |
Figure 1: Bar chart demonstrating the proportion of the 20 shortlisted projects which addressed each of Marmots six key principles.
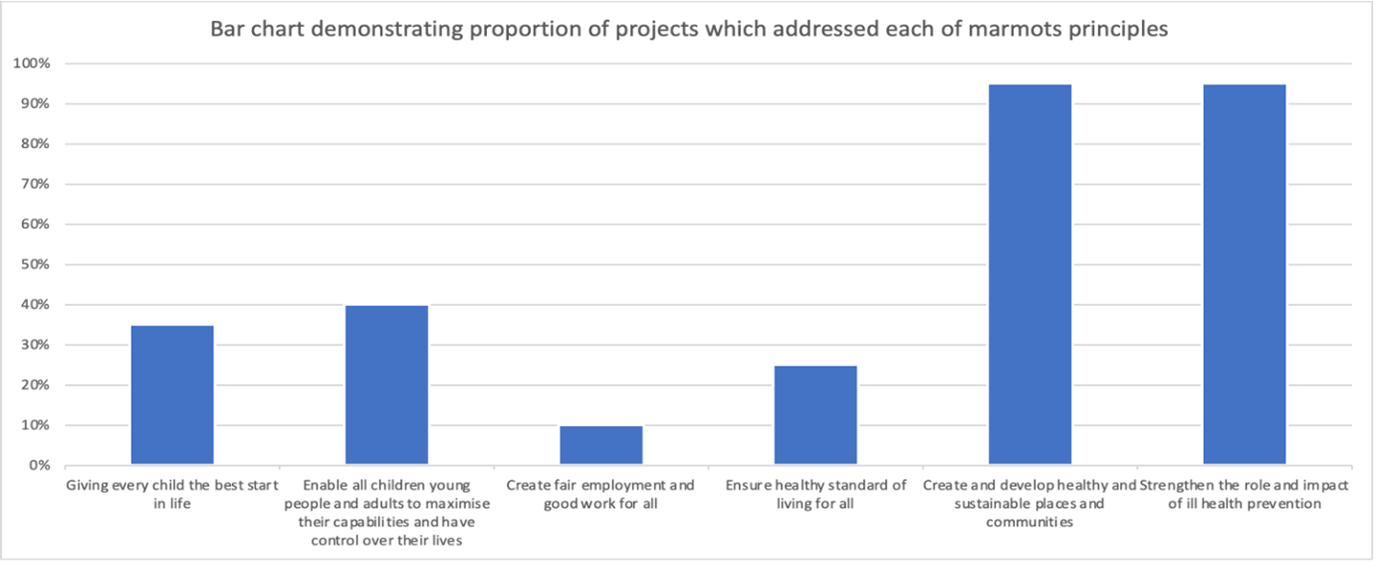
Figure 2: Bar chart demonstrating the proportion of the 18 non-shortlisted projects which addressed each of Marmots six key principles.