
Introduction
This report summarises the activities and support delivered to local systems in the first year of the support programme. It focuses on illustrating outputs and outcomes whilst recognising that the nature of the support provided will continue to deliver impact beyond the timeframe of this report.
The report will also illustrate our reflections and learning from this initial year and is presented to ensure clarity but also inform future delivery.
Overall, this has been a successful year for the programme. We demonstrate an effective programme start-up, good achievement against relevant KPIs, high levels of satisfaction with the support and a significant pipeline for Year 2. Our agreed aims, as well as our own knowledge and experience of sector needs, have been the drivers for our delivery.
We demonstrate through data, narratives and case studies how our approach has enabled local systems to understand their issues and challenges, getting to the root cause and evidence and taking a whole system approach to tackle these. The longer-term impact will be improved integration and better and more sustainable outcomes for local people.
Overview of the 2023/2024 BCF Support Programme
Key performance summary
The key performance highlights from the first year of the programme show the number of Health and Wellbeing Boards (HBWs), alongside the number of people the programme has engaged with.
Figure 1: Statistics on reach of our support
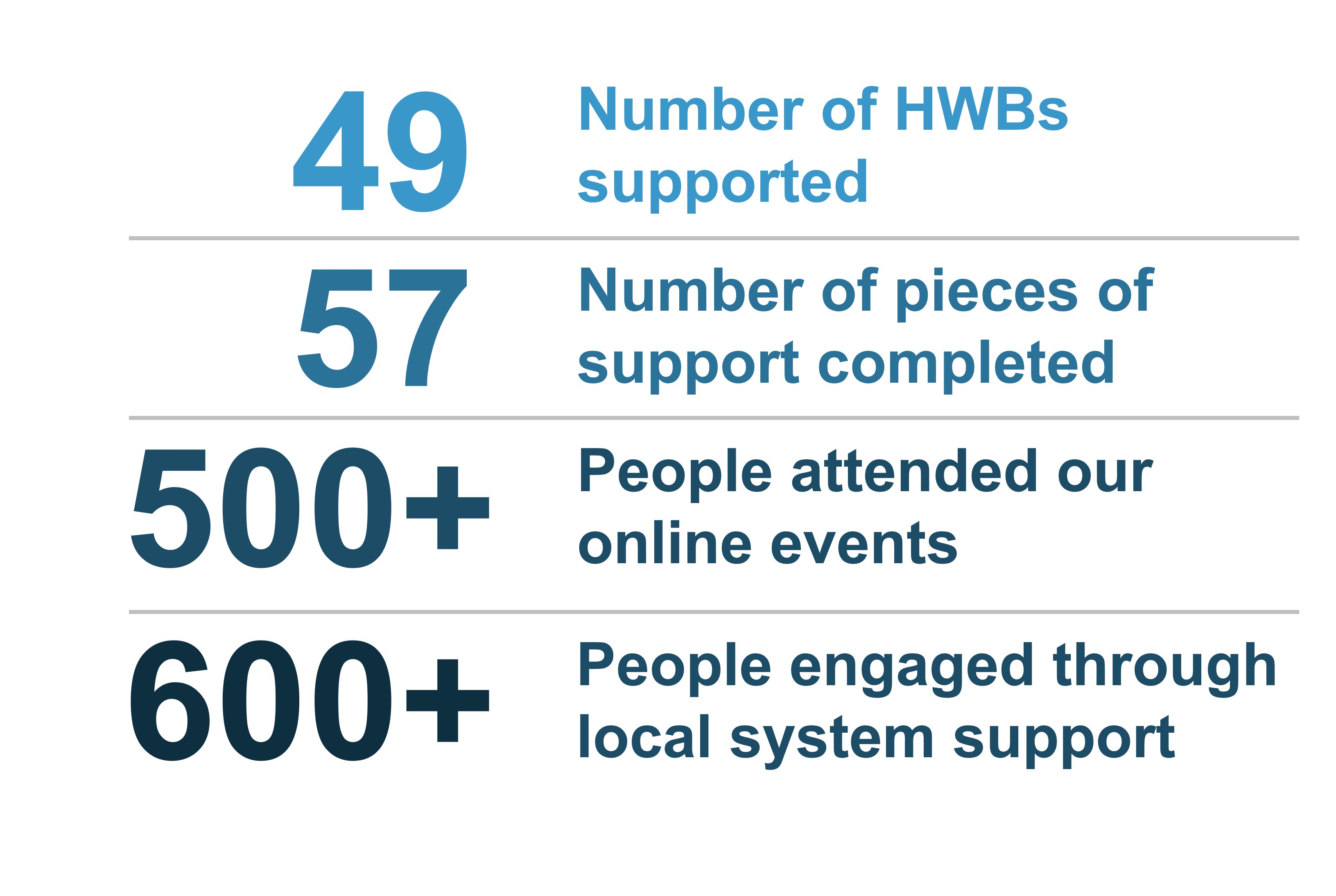
Figure 2: local authority regions supported
The BCF Support Programme provides support to local systems across England. The support is provided at a Health and Wellbeing Board level (HWB) and Integrated Care Board level (ICB).
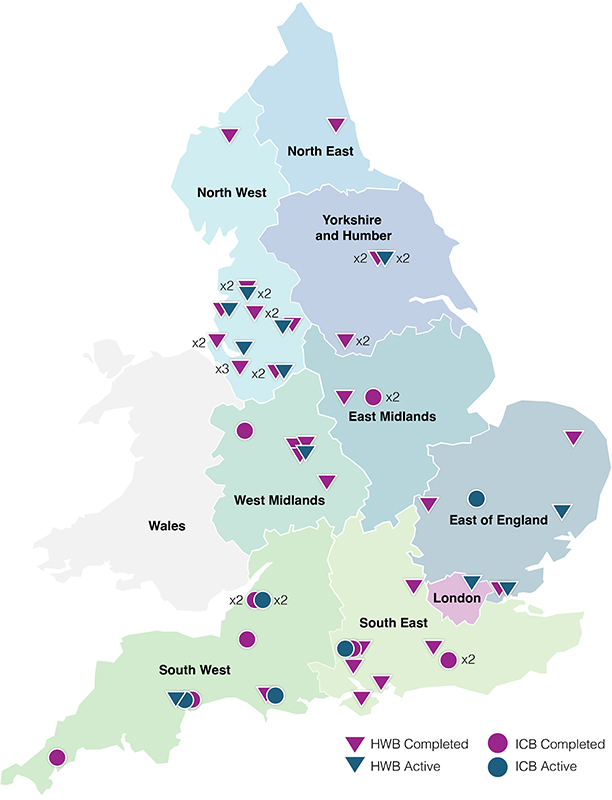
Figure 7: completed and active local system support BCF Support Programme 2023/2024
Local system support
Alongside the delivery, the first six months of the contract focused both on mobilisation of the programme and commencing support delivery to meet key performance indicators (KPIs) as outlined in the contract. Full details of the programme mobilisation activities were contained in the mid-year report. In summary, they included team recruitment, adapting processes and documentation, developing effective working relationships, procurement, branding, and marketing. This mobilisation ensured we had a strong foundation going forward. We also commenced delivery of specific system support during this period. In effect dual running the mobilisation and support.
At the time of the mid-year report, we had completed 16 local system support packages and had a further nine packages in delivery. Since then, local system support has ramped up. In total, we have completed or started 57 packages of support with a further 15 in the pipeline. This represents over a 120 per cent increase in the mid-year performance.
Graph 1: local system support 2023/24
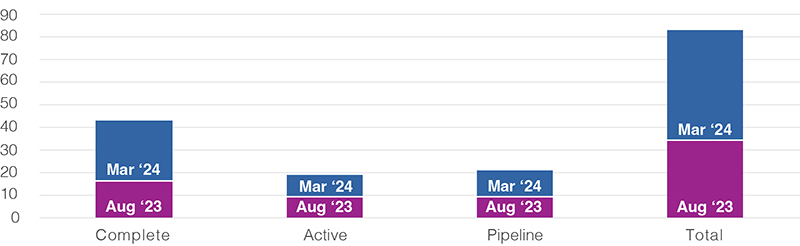
An image of a bar chart that shows the support by the BCF support programme, by status. An accessible version of the data can be seen in Table 2.
In line with our sector-led approach, all local system support has been scoped and developed with local systems, involving Better Care Managers and Care and Health Improvement Advisers, to ensure there is ownership of the support. Our trusted approach, to bring all stakeholder health and care organisations across a system together to agree on the challenges and support requirements, ensures that partners are engaged and bought into transformation activity.
In addition, we committed to deliver on the three outstanding Discharge to Assess (D2A) support pilots from the previous support programme’s agreement to deliver six D2A pilots and recruited three D2A pilot sites. Although these do not count towards the achievement of our KPIs in the current contract, team capacity and resources are utilised in delivering these pilots. We are gaining significant sector-wide insight and learning which supports the overall objectives of the BCF Support Programme. It is anticipated that these three pilots will be completed by July 2024.
Directed and non-directed local system support
Throughout the year we have worked closely with DSOG (Discharge Support Oversight Group) and other national BCF partners, taking their direction to specifically focus on the ‘discharge challenged’ local systems.
In total, we have engaged with 49 local systems (HWB level) and 43 of those have been at the direction of national BCF partners, representing 87 per cent.
Graph 2: directed and non-directed local system support
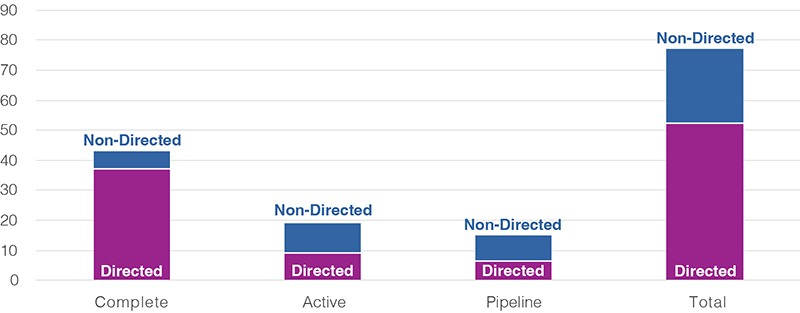
An image of a bar chart showing the breakdown of non-directed and directed support by status. An accessible version of the data can be see in Table 3.
Out of the 43 local system support being completed in Year 1, six support packages were non-directed bespoke support (around 14 per cent) and 37 packages delivered were directed and targeted support. Most of the targeted support was also directed.
Looking at only at the ‘active’ support (that is in delivery as of 31 March 2024) the proportion is higher, nine out of 19 ‘Active’ Local System support is non-directed (around 47 per cent).
Regional representation of local system support
At the time of the mid-year report, we had started support in seven of the nine regions, covering 30 health and wellbeing boards. We have now completed or started support packages in every region of the country covering 49 health and wellbeing boards.
Graph 3: local system support per region
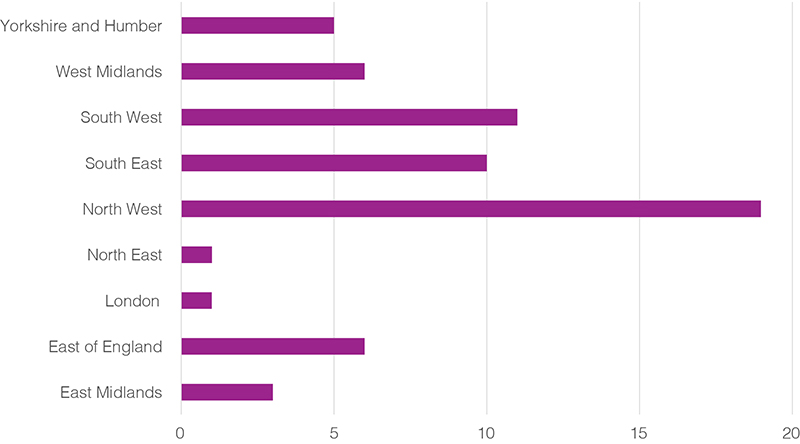
An image of a bar chart that show the number of systems supported by the nine local authority regions. An accessible version of the data can be see in Table 4.
Universal support
Our universal support offers to local systems provide a range of new and updated, evidence-based, interrelated guidance, learning and insights, tools and techniques that are universally applicable and transferable to the wide range of activities undertaken across the health and social care sector. These are delivered through tools such as the High Impact Change Model (HICM) for Managing Transfers of Care, online learning events, learning reports, workshops or masterclasses with expert speakers and sessions at national and regional conferences.
Graph 4: universal support 2023/24
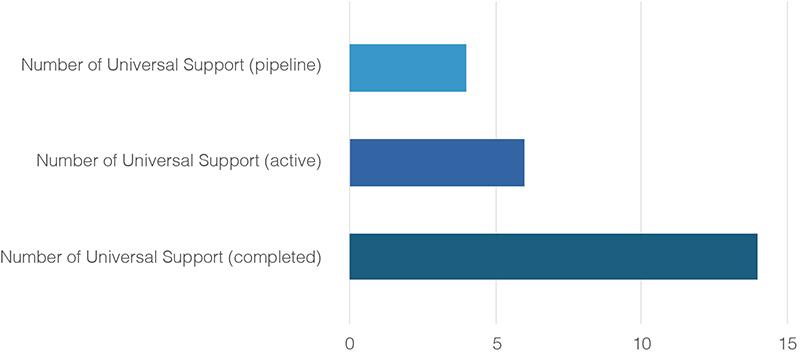
An image of a bar chart showing the number of universal support by status. A breakdown of the data can be seen in Table 5.
We have ensured the rapid development and delivery of the universal support offer. In addition to making the universal offer open to all, we also use these tools as part of our targeted or bespoke offer. We aim to continually refine and develop our universal support offers based on learning and evidence gathered.
Directed and non-directed universal support
Throughout the year we have worked closely with DSOG and other national BCF partners, taking their direction to provide universal support. In total, we have delivered 14 universal support offers in Year 1 and out of them, seven were directed (50 per cent).
Outputs, outcomes, and impact
Evaluation framework
We have produced an evaluation framework to help us understand, evaluate, and improve the effectiveness and efficiency of the support programme activities. This covers all our support classifications and distinguishes between short, medium, and long-term. Given the length of time the support programme has been operational, more data and information on outputs and shorter-term outcomes and impacts will emerge as the programme continues into Year 2.
An external evaluator, IPSOS, has been appointed and we are also working closely with them as requested.
Universal support tool and reports
Managing Transfers of Care – A High Impact Change Model: This work promotes a new approach to system resilience, moving away from a focus solely on winter pressures to a year-round approach to support timely hospital discharge. In addition to being a Universal offer, we have successfully utilised the High Impact Change Models (HICM) in our support to Local Systems. These short case studies illustrate how the HICM Model is used within the BCF Support Programme.
Discharge to Assess support offer: data analytics: The HICM has been used as the basis for the Improvement through Data module included in the D2A support offer. The module has been developed using the maturity levels in the HICM to identify challenges and produce suggestions for improvement. The first system the support programme will be working with using this approach is Dorset. This involves the development of a data working group which considers the available and desired performance information. Dorset data colleagues will be supported to join up their data sets and move towards 'One Version of the Truth' to get an informed overview of patient flow.
Capacity and demand planning capabilities - 19 health and care systems: We commissioned Changeology to provide targeted support to analyse capacity and demand planning capabilities across 19 health and social care systems (at HWB level). The objective was to understand the barriers and identify opportunities to improve capacity and demand planning capability to enhance overall system resilience. Part of this support included an assessment of the system's maturity against the 10 High Impact Changes in the updated model for managing transfers of care.
Online events: We have delivered seven online events covering areas such as capacity and demand planning, winter pressures, care transfer hubs, and began a programme of learning lunches. Average satisfaction across online events was 83 per cent with 97 per cent of respondents saying that the event met the objectives. Of the seven events delivered, the estimated attendance was almost 500 people of which 172 were from councils in England with adult social care responsibilities, representing 79 unique councils. Other organisations reached include NHS Trusts, ICBs, charities, universities and other government departments.
Graph 5: online event satisfaction
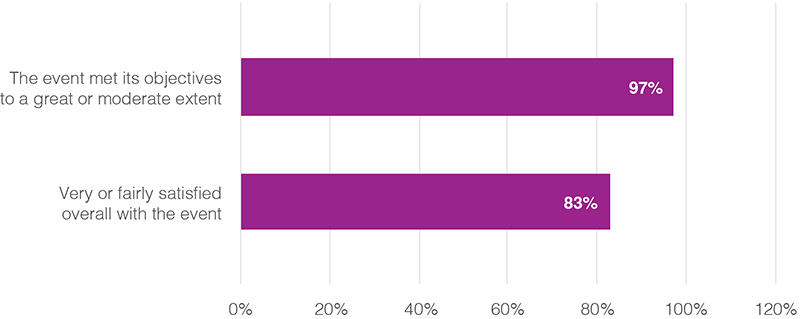
An image of a bar chart that shows the levels of satisfaction from survey responses in relation to the BCF Support Programme's online events. A breakdown of the data can be see in Table 6.
Learning lunch discharge to recover and then assess: Attended by over 150 people representing 80 NHS organisations and councils. Delivered by a national expert in the field. Covered an evidence-based, person-centred approach to hospital discharge assessment. Seventy eight per cent of attendees felt very satisfied to fairly satisfied with the event.
The speaker had a great deal of experience, was very upfront and honest. Very engaging and easy to listen to."
- Event participant
Capacity and demand planning - shifting concepts into practical applications: Delivered by national experts and attended by over 60 people covering capacity and demand planning, developing a management operating system, and learning capacity and demand lessons from others. Ninety one per cent of attendees felt the objective of the webinar was met.
I found the session really helpful and also to have the message reiterated that we are all learning about this together.
- Event participant
Universal support accessed via the BCF webpage
We launched the updated support webpage in January 2024 to make our Universal Support offers and tools available to health and social care systems nationwide.
We evaluate the usage of our webpage and whilst it is early days, we can already see that the tools are being accessed widely. In total, we have had over 1,500 views creating nearly 5,000 events (an interaction with the page, for example, clicking a link or downloading a PDF). We will continue to monitor the use of our website and identify ways we can increase usage and engagement time.
Targeted local system support
Targeted support examples include scoping diagnostic support, capacity and demand support, discharge to assess support and peer reviews. During this year, our focus has been mainly on targeted support. Scoping diagnostics and capacity and demand support accounted for over 50 per cent of the programme. This was significantly influenced by the number of directed support referrals. This is how we undertake this support:
Scoping diagnostic
Our scoping diagnostic process is a collaborative investment in a structured, joined-up, conversation with senior system leaders, led and managed by a senior expert. The objective is to build a shared understanding of the footprint, scale, complexity, capacity, and capabilities within the system. The conversations enable the system leadership to define and prioritise the support requirements for the system. The outcome is agreed support requirements and a joint compact for the delivery of bespoke support from the programme.
During the year we completed 15 diagnostics using this approach, which took less time to deliver and demanded fewer resources than the traditional peer review process but provided the opportunity for a more focused investigative process. We have had good feedback on this process, and some systems have reflected that the ability to test thinking collaboratively on an iterative basis led to deeper shared insight and agreement on issues and next steps. We are also pleased that, subject to some clear criteria, work of this nature has been recognised as a support in its own right. We are finding that as the challenges, complexity of support, and the need for pace of delivery increases, it is the collective reflection that brings partners together to enable shared understanding and whole systems approach to problem solving and planning rather than silo working. The support to York illustrates our approach.
Case study 1: Scoping diagnostic support in York
What issues did the system face? The system had shared goals and objectives and relationships between partners were developing well. They undertook an internal discharge stocktake in 2023 which had some positive impacts however there were significant gaps in the associated action plan and there was no system-wide discharge model. There was particular focus on Pathway 3, with patient flow and continuing healthcare processes being particularly challenged.
What support did the system receive? The system agreed a scoping diagnostic should be undertaken. This engaged system partners from the City of York Council, NHS Humber and North Yorkshire ICB, and the local acute trust. A series of iterative conversations, with individual stakeholders and as a collective, has led to a clear shared statement of challenges in the system and the associated support requirement.
What was achieved? As a result of the scoping diagnostic, two key support requirements were identified:
- the development of a jointly agreed implementation plan on discharge improvement, to deliver improved patient outcomes, reviewing the current assessment system, processes, and decision-making
- an agreed plan to implement transformation across Pathway 3, underpinned by jointly agreed principles and metrics to measure progress and improved outcomes. More people with complex needs are leaving hospital on the right pathway, receiving support that is right for them.
What happened next? As a result of the scoping diagnostic the system requested follow up support:
- discharge stocktake recommendation implementation
- place-based governance, and commissioning and finances review.
Peer review
The ethos of sector-led improvement is at the heart of our support programme, fostering the sharing of good practice, challenge, and solution among leaders within the sector. In Autumn 2023, we undertook a continuing healthcare (CHC) peer review in Sefton, led by peers with a range of experience and expertise, most of which were active in post from across the country. This review provided wide-ranging recommendations to improve CHC processes; develop a shared vision for CHC across the system; and improve communications. The review recommendations are being taken forward and the system has been offered a follow-up Peer Review to track progress and remaining gaps.
Capacity and demand planning
All local areas are required to agree and submit demand and capacity plans. This is a complex and challenging process. However, when a good plan is coupled with a good discharge to assess process which is owned by the whole system, it results in lower lengths of stay and delayed discharges but most importantly better longer-term outcomes for older people.
Our targeted capacity and demand planning support is a hands-on expert, critical friend model of support. The aim is to achieve a clearer understanding of the capacity and demand task, what the system needs to do to work with their data and to assemble an agreed picture and narrative. It also supports their building of the short-term and long-term action plans to make improvements stick. The outcome is a tangible difference for systems in gaining a detailed insight into current approaches to capacity and demand planning and any related challenges. It also supports the formulation of clear improvement recommendations to empower systems to learn how to improve the quality of future planning. We have shared our insights and learning about the core components of effective planning with DSOG. During 2023/24 we have undertaken 27 demand and capacity support packages.
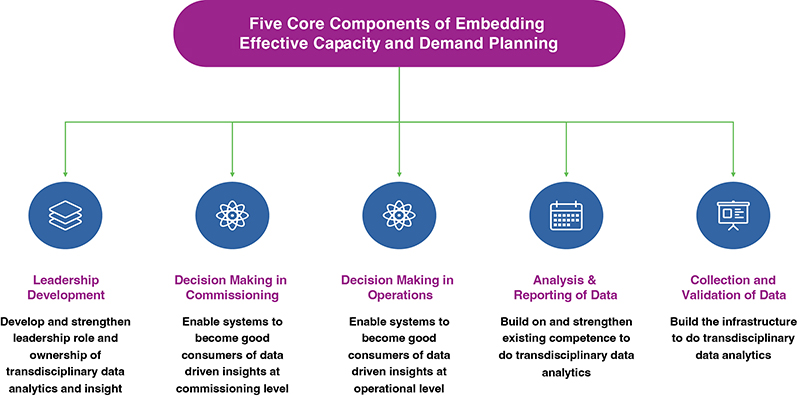
Figure 8 shows five circles with symbols in each. Circle 1, Leadership development; Circle 2, Decision making in commissioning; Circle 3 Decision making in operators; Circle 4 Analysis and reporting of data; Circle 5 Collection and variation of data.
Discharge to assess support offer
Our in-house discharge to assess (D2A) support is an analytical approach with four modules:
- Case review workshops: in-person audit of discharge cases with frontline staff, comparing actual and ideal patient outcomes and the reasons for the disparity between the two.
- Environment for change: a survey of frontline staff, establishing their perspectives on D2A and their organisational culture and capacity for change.
- Voice of the person: patient interviews on their experiences of discharge.
- Improvement through data: supporting colleagues in the system working in data to create a local data analysis, as well as identifying gaps and opportunities in the system’s data collection skills and processes to co-produce recommendations for improvement.
It is a diagnostic toolkit and framework used by the BCF Support Programme to work collaboratively with the local system to understand how well D2A is working and what the system’s environment for change is, before supporting the system to establish its shared priorities and take forward these priorities to make improvements. It aims to address the root cause of performance and outcomes issues in relation to the implementation of D2A.
In the local systems we have worked with, C&D and D2A are not just about data and numbers and shared evidenced-based insight but also cultural shifts, relationship building and leadership at the local and system level. The support provides systems with the processes and governance mechanisms to focus on planning and developing a sustainable home first model and consider shifting investment to more home-based and community-based provision, to enable more people to go home, and stay home, after hospital.
Case study 2: Capacity and demand planning support in Cornwall and the Isles of Scilly
What issues did the system face? The system was requested by the discharge support and oversight group to produce and submit an early draft of the intermediate care capacity and demand plan. The system had a good grip of the data and analytics to understand the issues and challenges but did not have a shared process to come together to discuss and agree the actions required to address the challenges.
What support did the system receive? Three focused discussion clinics were held with health and social care partners to provide the platform to review, discuss, debate and agree short-term and long-term actions. The discussion clinics supported the system partners to come together and focus on discussing and agreeing improvement actions.
What was achieved? The system was able to make the shift and interpret the good data and analytics towards a single narrative and improvement delivery plan (short-term and long-term) for demand and capacity challenges and for intermediate care more widely. The recommendations and suggested priorities built on the existing draft intermediate care strategy and pulled together several existing plans and programmes in the system to become the first draft of a joint overarching plan.
What happened next? The system welcomed the support. The system received positive feedback on its capacity and demand narrative and plans from DHSC and DSOG.
Bespoke local system support
The bespoke support offers are developed in close collaboration with each local system, as part of the support definition process and/or the more in-depth scoping diagnostic support. The visual below highlights the range of bespoke support we offer.
Figure 9: examples of bespoke support areas
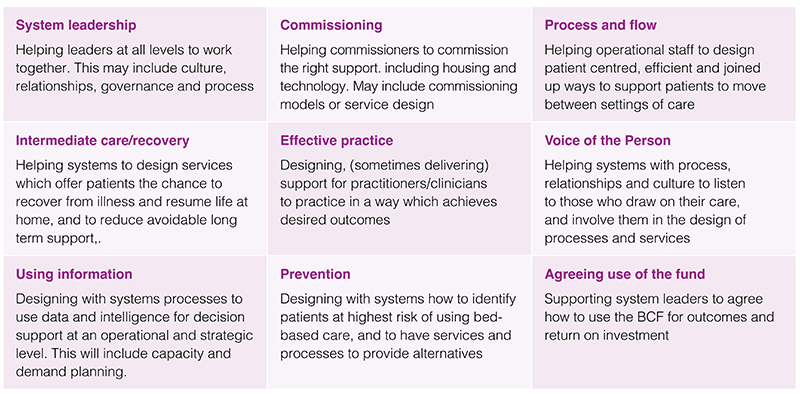
Figure 9 shows nine box with short information on each example of bespoke support provided through the programme.
- System leadership: Helping leaders at all levels to work together. This may include culture, relationships, governance and process
- Commissioning: Helping commissioners to commission the right support. including housing and technology. May include commissioning models or service design
- Process and flow: Helping operational staff to design patient centred, efficient and joined up ways to support patients to move between settings of care
- Intermediate care/recovery: Helping systems to design services which offer patients the chance to recover from illness and resume life at home, and to reduce avoidable long term support
- Effective practice: Designing, (sometimes delivering) support for practitioners/clinicians to practice in a way which achieves desired outcomes
- Voice of the person: Helping systems with process, relationships and culture to listen to those who draw on their care, and involve them in the design of processes and services
- Using information: Designing with systems processes to use data and intelligence for decision support at an operational and strategic level. This will include capacity and demand planning.
- Prevention: Designing with systems how to identify patients at highest risk of using bed-based care, and to have services and processes to provide alternatives
- Agreeing use of the fund: Supporting system leaders to agree how to use the BCF for outcomes and return on investment
Examples of bespoke support areas
System leadership
Helping leaders at all levels to work together. This may include culture, relationships, governance and process.
Commissioning
Helping commissioners to commission the right support. including housing and technology. May include commissioning models or service design.
Process and flow
Helping operational staff to design patient centred, efficient and joined up ways to support patients to move between settings of care.
Intermediate care or recovery
Helping systems to design services which offer patients the chance to recover from illness and resume life at home, and to reduce avoidable long term support.
Effective practice
Designing (sometimes delivering) support for practitioners or clinicians to practice in a way which achieves desired outcomes.
Voice of the person
Helping systems with process, relationships and culture to listen to those who draw on their care, and involve them in the design of processes and services.
Using information
Designing with systems processes to use data and intelligence for decision support at an operational and strategic level. This will include capacity and demand planning.
Prevention
Designing with systems how to identify patients at highest risk of using bed-based care, and to have services and processes to provide alternatives.
Agreeing use of fund
Supporting system leaders to agree how to use the BCF for outcomes and return on investment.
The following two case study examples illustrate how the BCF Support Programme works with local systems to scope the support requirements and then create a package of bespoke support that meets the system’s challenges. This sector-led approach maximises buy-in from systems and helps ensure the most effective support delivery.
Case study 3: Leadership and managing out of hospital demand support in Bristol, North Somerset, and South Gloucester ICS
What issues did the system face? A BCF Scoping Diagnostic undertaken in 2022/23, identified the challenges of a complex system with emerging system governance. The system had not yet built enough trust and confidence around and within its D2A transformation programme, to move forward in a cohesive way. Leadership behaviours and organisational culture were impacting on the improvement journey. The system did not fully understand its community demand and capacity and there was no consistent overall understanding of flow across the whole system and the interrelated nature of capacity.
What support did the system receive? Following agreement from system leaders, the BCF Support Programme arranged two packages of bespoke support covering leadership, culture and learning and demand and capacity planning.
What was achieved? The support offer is progressing as expected with buy-in from senior leadership. The capacity and demand tool is nearing completion and will be handed over to system colleagues in April 2024.
What happened next? A final leadership workshop is scheduled to agree a memorandum of understanding on ways of working later in April.
Case study 4: Pathway mapping and BCF pooling of budgets support in Cheshire West
What issues did the system face? Following a scoping diagnostic the system agreed that they needed support to improve their understanding of:
- the current pathway landscapes
- how potential changes could impact patient outcomes and flows
- the impact on finances and commissioning practices.
What support did the system receive? Support was commissioned from ARCC and Changeology who undertook an analysis of the systems discharge pathways. Involved process mapping with stakeholders, management operating system analysis and a collaborative workshop.
What was achieved? As a result of the support the system amended the daily triage meeting – seeing an improvement in flow. They started to develop a joint governance structure around community providers and home first and began to see a cultural shift in relationships. The work also highlighted to partners that more social care input is needed prior to discharge. 100 per cnet satisfied with the support and the final outputs.
What happened next? System leadership is convening to discuss how best to embed the findings, using this work as an opportunity to drive change.
Evaluation of targeted and bespoke support
Evaluation
We implemented our evaluation framework and undertook the following activities:
- surveys
- wash-up calls
- end of support reports.
Overall satisfaction with the local system support received by systems was positive and most agreed or strongly agreed that the support met its objectives and that they were very satisfied or fairly satisfied with the support they received. Respondents were only asked whether they felt the support was a good use of time and resource in quarter four so an average is not available for the full year. However, in quarter four, 83 per cent of respondents said the support was a good use of time and resources.
Survey responses to questions about meeting objectives and overall satisfaction with the local system support received (percentage of respondents).
Graph 6: local system support satisfaction

An image of a bar chart that show the levels of satisfaction from survey responses in relation to the BCF Support Programme's local system support.
Impact
Survey respondents are asked to provide the key benefits they anticipate from the support for their local health and social care system. Key benefits of the support included better quality relationships and joint working, clarity around strategy, and clear identification of focus areas and future work. Specifically, local systems highlighted the following outcomes as a result of the support provided:
- improved rational and knowledge-based expertise
- aligned plan with strategy; clear pathway for implementing change
- improved assurance and governance
- moving BCF spending to a more strategic footing
- improved relationship between ICB and Alliance
- moving towards joint commissioning
- identification of clear areas for future working
- improved understanding of partner views through joint sessions
- sharing good practice
- new focus on managing demand as well as capacity
- whole system working toward the same aim
- one version of the truth regarding the data and intelligence
- agreed focus areas to be addressed in the short term to support flow.
Sharing insight and learning
Our support work in 2023/24 has revealed several consistent wider learning themes facing the health and care sector. The first year of our support delivery activity has added to our bank of knowledge and insights about Local Systems and the wider sector.
We have actively disseminated and shared this learning through a variety of channels:
- blogs on the BCF webpage
- online learning lunches
- newsletters, bulletins and social media
- in-person sessions at national conferences
- the Scoping Diagnostic Learning Report (Universal Support)
- verbal and written updates to national partners
- internal communication at the LGA, for example to LGA policy colleagues.
A few of the key learning themes we have learned:
Leadership and relationships
- Our scoping diagnostics activity has identified that system leaders often require expert support to bring partners together and enable a whole system approach to consider and determine the current state analysis and to scope out areas of support needs. It may also be necessary to support the development of an agreed and owned vision if one does not exist.
- When we support the review of BCF plans plus the insight from our leadership support offer we often see that relationships are challenged between health and care partners within a system. Whilst our technical support adds real value it is often further enhanced with support to system leaders to improve culture and ways of working. This enables constructive engagement with the findings and recommendations from the support, which in turn develops a ‘single version of the truth’ approach and commitment to the next steps to deliver sustainable improvement.
Intensive, in-depth support
- Due to the challenges, capacity and capability issues faced by local systems, the requested support requirements are intensive, root and branch appraisals of culture, behaviour, governance, processes, and practice. This needs expert input from larger consultancy organisations, to establish the current state, next steps and most importantly how to deliver change and improvement.
- Insights from our capacity and demand planning support reveal that identifying root causes and producing effective and deliverable plans are multi-faceted. This requires the development and embedding of a whole systems management operating model. To have the maximum impact, this must be complimented by a programme of learning and development for leaders and staff at all levels in the system. The aim is for everyone to understand the building blocks and benefits of the approach and thereby improve practice in this area.
Relationships between some ICBs and local authorities
- There are significant financial, and operational challenges across all organisations (NHS and local authorities) that make up integrated care systems (ICSs). In addition, the ICSs are still maturing including determining the approach to delegation at place. This combination of complex challenges is creating tensions in the relationships between some ICBs and their local authority partners in the system. Local systems are increasingly asking for support around resolving mutual financial pressures, agreeing their overall BCF priorities and plans, and agreeing what is best done at place or ICS level.
Data and information sharing
- Typically, local systems are struggling to create effective means of using data to support better capacity and demand planning, with blame often being attributed to technical issues, either in terms of the technology involved or legal concerns about data sharing. All the areas we have worked with, wanted to establish some sort of shared pool of information. Many areas also highlighted a desire to make more of the data they already have, with issues around the creation of real-time data for operational use, as well as poor data quality across organisations or sectors.
Person-centred approach
- The D2A pilots have identified that some local systems do not have the building blocks in place to be as person-centred as they need to be. The infrastructure and processes are not in place to consistently capture and reflect the voice of the person receiving services and understand the link between procedure and patient outcomes. As with the learning from the capacity and demand support, there are systemic gaps in joined-up data review and analysis.
Delivering improvement support
- For support to have impact, a local system needs to be aligned with a common understanding of their challenges and their support requirements. We have also learned that local systems take and need time to engage with support specification and delivery due to capacity gaps and their challenging operational environment. In addition, the number of support offers available, whether commissioned centrally or by local systems themselves, can lead to some systems feeling overwhelmed and unsure about how the BCF support element can best add value. This latter issue could be mitigated by having clearer joint support coordination at a regional level.
- We have also learned that some systems, when faced with numerous pressing challenges, generate an ever growing list of unprioritised and disparate activities. This leads to an ever-growing list of unprioritised initiatives. Systems often need support to develop and consider their own evidence and intelligence to enable them to prioritise, and design a robust and evidence-based change programme.
Building on learning
Our support work in 2023/24 has revealed several consistent wider learning themes facing the health and care sector. We will use this wider learning in the delivery of our support in Year 2.
System-level relationships
The need to develop and deliver a shared vision is crucial. Some systems have been unable to align behind a single wholly owned vision and consequently haven’t moved into the delivery phase. Moving into 2024/25 the support offer around leadership should remain key to supporting these systems.
Data and information
As highlighted above, all health and social care systems need good-quality data to inform their operations. Typically, systems are struggling to create effective means of using data to support these aims. High-quality data also supports our work within the BCF Support Programme, feeding into our support offers around discharge to assess, and capacity and demand planning. We are also developing a number of universal support packages around capacity and demand planning, D2A and data support which will support systems going forward.
Capacity and demand modelling
As already noted earlier in this annual report, a consistent theme was a request for support with understanding the demand and capacity of the system, and particularly the capacity of services available in the community. If systems do not understand their capacity and demand it is very challenging to improve flows and deliver the best outcomes for people. Our targeted support offer around demand and capacity modelling will provide further insight and learning and coupled with our webinars and masterclasses, will continue to enhance the support to systems into 2024/25.
Looking ahead to year 2
As we look forward to the second year of the support programme we will build on the successes and lessons learned from the first year. We have significant demand for our support in 2024/25, outstripping the current budget. This is positive in that it shows the value of the support being offered by this programme, but we recognise that we need to prioritise, and are already working with the authority to do this.
In Year 2, we will work with partners to ensure that support is aligned and targeted at those most in need of it. We will continue to adapt our approach to the sector’s needs and to national policies and priorities. We will share our insights and learning more frequently and widely. Our aim at the end of Year 2 is to leave a strong legacy of tools, system capability, and knowledge about evidence based change.