The new Dynamic Support Register and Care (Education) and Treatment Review policy and guidance was published in January 2023 and aims to prevent unnecessary hospital admissions and detention under the Mental Health Act for people with a learning disability and autistic people. It refreshes the Care (Education) and Treatment Review policy and guidance and for the first time combines this with the first published national Dynamic Support Register policy and guidance, linking these tools so neither are seen in isolation.
Introduction
The new Dynamic Support Register and Care (Education) and Treatment Review policy and guidance was published in January 2023.
The policy aims to prevent unnecessary hospital admissions and detention under the Mental Health Act for people with a learning disability and autistic people.
The new policy refreshes the Care (Education) and Treatment Review policy and guidance and for the first time combines this with the first published national Dynamic Support Register (DSR) policy and guidance, linking these tools so neither are seen in isolation.
The policy has been co-produced with people with a learning disability and autistic people.
Definitions
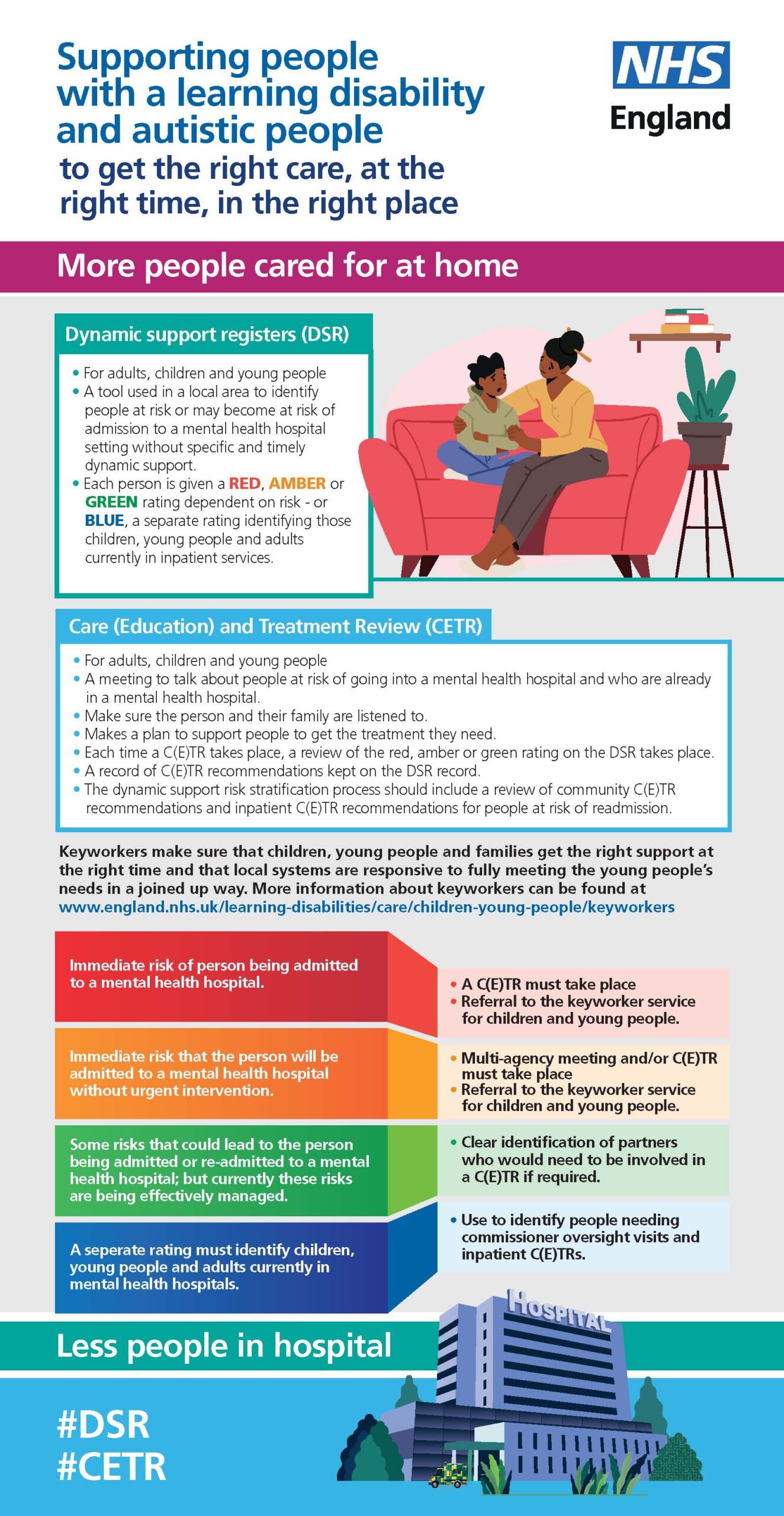
- A Dynamic Support Register (DSR) is a list of people with a learning disability and autistic people who need support because they at risk of going into hospital if they do not get the right care and treatment in the community.
- A Care and Treatment Review (CTR) makes sure adults get the right care and treatment and looks at how to make care and treatment better for adults. A CTR is for people who are at risk of going into hospital or who are already in hospital, which includes: children; young people; adults with a learning disability or autism.
- A Care (Education) and Treatment Reviews (C(E)TR) is different to a CTR because it is for children and young people and includes their education needs. C(E)TRs are independent meetings about someone’s care and treatment run by a C(E)TR panel which includes people who are not involved in their everyday care to ensure independence, including experts by experience.
Background
Following the publication of the Building the Right Support Action Plan, the guidance for DSRs and C(E)TRs has been refreshed and bought together into a single document.
- Community C(E)TRs and DSRs are tools to help prevent the inappropriate admission of people with a learning disability and autistic people to a mental health inpatient bed, including specialist hospitals.
- Inpatient C(E)TRs are used when an admission is appropriate to regularly review the quality of care and treatment provided to individuals and will include preparation for discharge.
The refreshed policy and guidance reflects the learning from the National Safe and Wellbeing Review Programme December 2021 and the proposal to put C(E)TRs and DSRs onto a statutory footing as part of the proposed reforms of the Mental Health Act (1983). In response to the learning from the Safe and Well Review Programme there is an increased focus on quality of life and how physical health needs are met. In future C(E)TRs will include a new question on quality of life and a strengthened focus on participation in meaningful activity.
Key changes in the policy and guidance
The new policy links DSRs with the C(E)TR policy for the first time.
To establish greater consistency, in how DSRs are managed and used, the guidance includes new minimum standards for DSRs. These include defining who should be included in the DSR and how risk should be stratified including a unified system for colour coding risk level. It also gives people and families the right to request to be included on the DSR list.
The policy says that ICBs (Integrated Care Boards) should set out a process explaining how someone, or others around the person, can request to be included on the DSR and the criteria for inclusion.
Anyone can ask for a community C(E)TR, but people should only get a C(E)TR if their support needs show it is right for them and they are at risk of going into hospital.
For someone to go on the DSR they would have to give their consent.
The policy states that the DSR should use the following colour coding to reflect risk:
- Red is for people who are at high risk of going into hospital straight away
- Amber is for people who are at high risk of going into hospital if they do not get the right care and treatment soon
- Green is for people who are having their risks managed well at home
- Blue is for people who are already in hospital
The guidance clarifies when C(E)TRs should happen. The new policy says that a C(E)TR should be set up:
- six weeks after someone goes into hospital if someone has already had a C(E)TR in the community
- if they go to another hospital or move to a ward in the same hospital with higher or lower security
- if a person finds out they are autistic or have a learning disability when you are in hospital or after you leave hospital
- if a clinical review shows that someone is not autistic or do not have a learning disability when they have been told before that they are autistic or have a learning disability.
The Key Lines of Enquiry (KLOEs) for C(E)TRs have been expanded to ensure that there is greater focus on checking that physical health needs are being met and individuals have access to meaningful activities.
Every time someone has a C(E)TR the DSR should be updated to show if their risk of going to hospital has changed and a record of what was agreed at the C(E)TR is kept on the DSR records.
Key issues for Integrated Care Boards
The refreshed guidance places responsibility on ICBs to ensure that DSRs and C(E)TRs are embedded in their multi-agency work to prevent admissions to mental health inpatient beds and reduce length of stay.
As well as commissioning community services that help people with a learning disability and autistic people live good lives in their local community.
It sets out the expectation that ICS (Integrated Care System) senior leadership will have oversight of delivery and quality of DSRs and C(E)TRs. Executive leads (chief nurse or executive director for commissioning) must have oversight of the local DSRs and ensure effective collaboration between health organisations and local authority partners.
The guidance expects ICBs to establish a C(E)TR oversight panel to review the C(E)TR of people for whom there is concern. Its membership should include the ICS medical director, senior responsible officer, and a senior social care representative.
The guidance expects that responsible commissioners from local provider collaboratives and the ICS, including local authority joint commissioning services, should facilitate access to appropriate advocacy support for people before, during and after C(E)TR. This can include the use of family advocates.
Next steps for councils
Where a council is providing leadership to joint commissioning arrangements for mental health, learning disability, autistic people and/or Special Educational Needs and Disabilities (SEND) they will want to ensure that commissioners are taking action to implement the guidance and that governance arrangements within the ICS reflect the requirement for regular reviews of the DSR and a C(E)TR oversight panel.
All councils can identify senior commissioners and practitioners to participate in the further development of the DSR to ensure that there is a shared social care, education and health view on which individuals are at risk of admission and the level of risk and work with health colleagues to develop plans to help people avoid an admission. These plans will include NHS community services, including adapted mental health services, alongside the education, care and housing provision required to avoid an inpatient admission.
Where possible, people who are inpatients or at high risk of an admission will need to have a named social worker who will participate in C(E)TRs. Social workers can bring their professional expertise and experience to discharge planning to ensure that risk is managed in the least restrictive way possible in the community.
Arrangements will be needed to ensure that people have access to an independent advocate to support them through C(E)TRs.
Advocacy organisations can be regularly briefed on developments in C(E)TRs and DSRs.
Councils can clarify routes for escalating safeguarding concerns identified through C(E)TRs in the community or in an inpatient setting, clarifying the role of each agency and the local safeguarding board(s).
Further information
- Dynamic support register and Care (Education) and Treatment Review policy and guide
- Easy read version of the policy
- Plain English version of the policy
- An infographic summarise the key points of the new policy
- Examples of successful community support for people with a learning disability and autistic people are Home For Good: Successful community support for people with a learning disability, a mental health need and autistic people (Care Quality Commission)
- Cawston Park Safeguarding Adults Review (SAR) Joanna, Jon, and Ben, published September 2021, Norfolk Safeguarding Adults Board relates to the death of three young adults with a learning disability and led to Safe and Well reviews and particular the stronger focus on the physical health of people in inpatient settings.)
- Responsible commissioner guidance - Who pays
- NHS Provider led DSR example: NHS England Dynamic Support Database and clinical support tool
- Regional Launch Webinar NDTi | C(E)TR DSR Policy Update 21 February 2023
{kind=link}