This case study forms part of the publication, Bespoke support for people with learning disabilities and autistic people, an evaluation on the impact consequence for local authorities and councils of delivering bespoke support to autistic people and people with a learning disability, including people who have been detained under the Mental Health Act (or at risk of being detained).
A young lady called Cara was brought to the provider’s attention by local commissioners. She was described as being ‘ready for discharge’. She had experienced multiple failed community provider placements and had kept being re-admitted to hospital.
The commissioners assisted with sourcing a property for Cara at short notice to facilitate a quick discharge. Cara is autistic. She had experienced lots of complex trauma, with self-harming behaviours. Due to the pressure to discharge her quickly from the hospital setting, Cara was discharged quickly into her new home, but it was far too fast for her and quite a challenging process. Cara had a history of ‘bouncing in and out’ of hospital, and Seco support was told it would be the 10th provider organisation supporting Cara out of hospital into the community. There were clear expectations from the professionals involved that the discharge would fail quickly, and Cara would most likely end up back in hospital. It has not been perfect and there are still challenging days, but Cara has been out of hospital for over 18 months now.
Costings were agreed when Cara was 17 years old, and Seco support was told to expect to renegotiate fees after Cara’s 18th birthday when she would come under adult social care. This can be a barrier for many organisations that are invited to start supporting a young adult prior to their 18th birthday, because there is no guarantee of continuity of funding once they transition to adult social care.
Seco support had to challenge the funding position in order to allow Cara’s support to continue past her 18th birthday. Seco support was the first provider that had worked with Cara and not given up on her. This is the strength of the relationship model.
Cara’s support is very complex in terms of the high levels of support she needs, and the risks which are often present around her behaviours. Cara has a community Deprivation of Liberty Safeguards (DoLS) authorisation in place so that her support team is able to keep her safe during times of challenge.
The quality of Cara’s relationships with her family, friends and support team is what is keeping her in the community. She is doing incredibly well and has not needed to be re-admitted to hospital for the past 18 months.
Cara’s funding was approved and contracted with Seco support via a spot purchase arrangement because they weren’t on the local authority framework agreement.
In other areas, Seco support works with personal budgets alongside families and also work off-framework where there is not an existing contracting arrangement in place.
In the provider’s experience, wraparound support from community health teams is usually good during transition from hospital to community and immediately after discharge within a couple of weeks; but following that it is lacking and there is often confusion about who is providing support. There needs to be a clear plan and a key point of contact from community teams to provide consistency to the person. There also needs to be continuity of information and support for the person, to the prevent the need for repeated assessments and revisiting trauma.
Seco support works with a relationship-based model. It recruits staff alongside the person and their family, using matching tools. A lot of emphasis of the model is on the support team and the property being bespoke to the person. Environment plays a big part in getting the support right. As a provider organisation it is able to work alongside people with complex and challenging needs but the key ingredient is about getting the support right.
Housing and accommodation solutions for the people they support tend to be single occupancy. One manager is allocated per service. Support staff don’t wear uniforms or lanyards. They don’t carry keys on their belts. The staff work together with the person they support to facilitate a good life in the community. A lot of training the staff receive is relating to person-centred values and approaches to support.
The provider often finds that there are demands from commissioners to discharge the person quickly, without a recognition of the need to go at the pace of the person. Seco support aims to stop the revolving door into hospital with good planning, good transition and building trusting relationships with the person and their families- acknowledging that they have experienced a lot of trauma. There is often an assumption that people with complex needs require a registered care setting, but bespoke support and housing solutions can absolutely work for people with complex needs.
The families are a key part of the process as they are able to provide rich information and insight about the person. The provider works towards the REACH standards for independent living as a set of standards for getting the support and the housing arrangements right for the person.
They use a detailed cost matrix for ISF and personal budget arrangements so that all of the budget spend is completely transparent. Their experience is that personalised funding arrangements work well as long as they are managed well, and from the right value base. It is difficult when terminology around personalised funding and personalised planning varies from area to area around the UK, so there is often confusion between providers and local authorities.
As an organisation, their first contract was an individual referral for a young adult who the funding authority had been unable to source a provider for. Once they were able to demonstrate the bespoke model of support worked well, they began to receive further referrals for individuals in long stay hospital and prison settings. Many people referred to them had experienced multiple provider placement failures and subsequent trauma as a result.
From the provider’s perspective, there are clear workforce pressures within local authority and health teams. There is a clear shortage of staff within adult social care teams and this is having a direct impact on systems and processes. Everything seems to be taking longer, many providers are handing back services, and local authorities seem to be orientated towards crisis response.
As a provider, Seco support have received ‘Good’ rating in all KLOE areas of their CQC inspection.
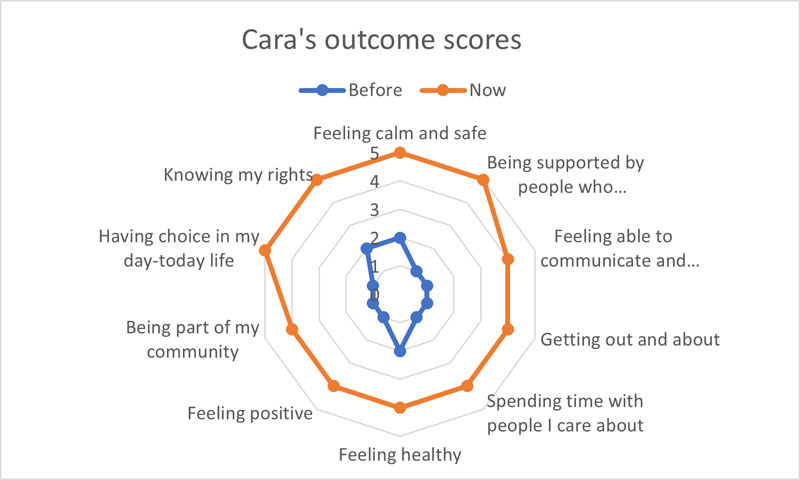
feeling calm and safe 2 before and 5 now.
being supported by people who understand me well 1 before and 5 now.
feeling able to communicate and being listened to 1 before and 4 now.
getting out and about 1 before and 4 now.
spending time with people I care about 1 before and 4 now.
feeling healthy 2 before and 4 now.
feeling positive 1 before and 4 now .
being part of my community 1 before and 4 now.
having choice in my day-to-day life 1 before and 5 now.
knowing my rights 2 before and 5 now.